

In-hospital Outcomes of Infective Endocarditis from 1978 to 2015: Analysis Through Machine-Learning Techniques
- PMID: 35198933
- PMCID: PMC8843990
- DOI: 10.1016/j.cjco.2021.08.017
In-hospital Outcomes of Infective Endocarditis from 1978 to 2015: Analysis Through Machine-Learning Techniques
Abstract
Background: Early identification of patients with infective endocarditis (IE) at higher risk for in-hospital mortality is essential to guide management and improve prognosis.
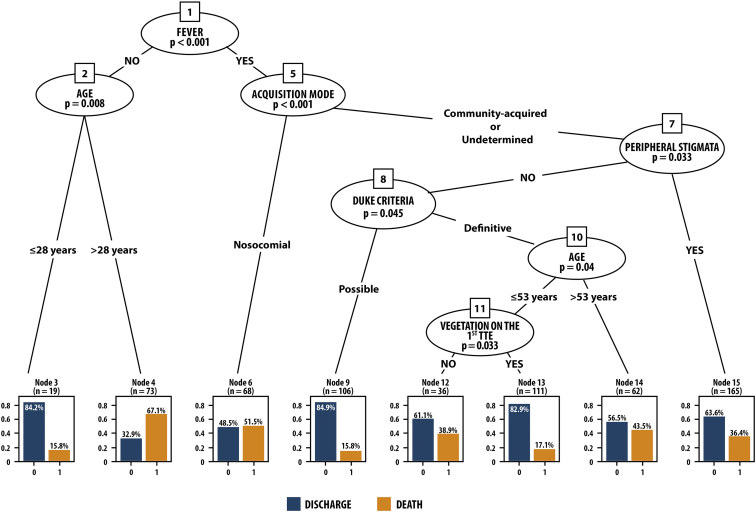
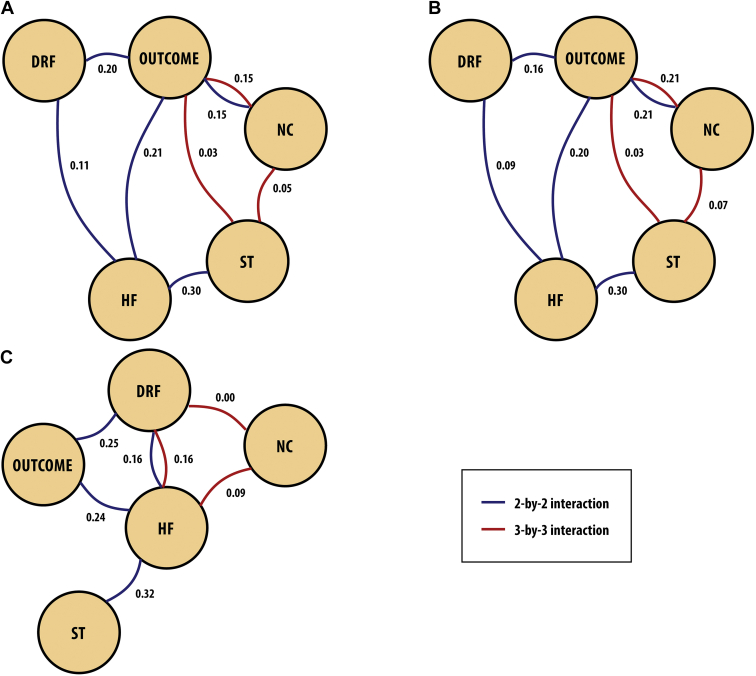
Methods: A retrospective analysis was conducted of a cohort of patients followed up from 1978 to 2015, classified according to the modified Duke criteria. Clinical parameters, echocardiographic data, and blood cultures were assessed. Techniques of machine learning, such as the classification tree, were used to explain the association between clinical characteristics and in-hospital mortality. Additionally, the log-linear model and graphical random forests (GRaFo) representation were used to assess the degree of dependence among in-hospital outcomes of IE.
Results: This study analyzed 653 patients: 449 (69.0%) with definite IE; 204 (31.0%) with possible IE; mean age, 41.3 ± 19.2 years; 420 (64%) men. Mode of IE acquisition: community-acquired (67.6%), nosocomial (17.0%), undetermined (15.4%). Complications occurred in 547 patients (83.7%), the most frequent being heart failure (47.0%), neurologic complications (30.7%), and dialysis-dependent renal failure (6.5%). In-hospital mortality was 36.0%. The classification tree analysis identified subgroups with higher in-hospital mortality: patients with community-acquired IE and peripheral stigmata on admission; and patients with nosocomial IE. The log-linear model showed that surgical treatment was related to higher in-hospital mortality in patients with neurologic complications.
Conclusions: The use of a machine-learning model allowed identification of subgroups of patients at higher risk for in-hospital mortality. Peripheral stigmata, nosocomial IE, absence of vegetation, and surgery in the presence of neurologic complications are predictors of fatal outcomes in machine learning-based analysis.
Contexte: Le dépistage précoce des patients atteints d’endocardite infectieuse (EI) présentant un risque élevé de mortalité à l’hôpital est essentiel pour orienter la prise en charge et améliorer le pronostic.
Méthodologie: Une analyse rétrospective a été réalisée sur une cohorte de patients suivis de 1978 à 2015 et classés selon les critères de Duke modifiés. Les paramètres cliniques, les données des échocardiographies et les hémocultures ont été évalués. Des techniques d’apprentissage automatique, comme l’arbre de classification, ont été utilisées pour expliquer l’association entre les caractéristiques cliniques et la mortalité hospitalière. De plus, le modèle log-linéaire et la représentation graphique en forêts aléatoires ont été utilisés pour évaluer le degré de dépendance entre les résultats hospitaliers et l’EI.
Résultats: Cette étude a permis d’analyser 653 patients : 449 (69,0 %) avec une EI avérée; 204 (31,0 %) avec une EI possible; âge moyen de 41,3 ± 19,2 ans; 420 (64 %) étaient des hommes. Mode d’acquisition de l’EI : communautaire (67,6 %), nosocomial (17,0 %), indéterminé (15,4 %). Des complications sont survenues chez 547 patients (83,7 %), les plus fréquentes étant l’insuffisance cardiaque (47,0 %), les complications neurologiques (30,7 %) et l’insuffisance rénale dépendante de la dialyse (6,5 %). La mortalité hospitalière était de 36,0 %. L’analyse de l’arbre de classification a permis d’identifier des sous-groupes présentant une mortalité hospitalière plus élevée : les patients présentant une EI communautaire et des stigmates périphériques à l’admission; et les patients présentant une EI nosocomiale. Le modèle log-linéaire a montré que le traitement chirurgical était lié à une mortalité hospitalière plus élevée chez les patients présentant des complications neurologiques.
Conclusions: L’utilisation d’un modèle d’apprentissage automatique a permis d’identifier des sous-groupes de patients présentant un risque plus élevé de mortalité à l’hôpital. Les stigmates périphériques, l’EI nosocomiale, l’absence de végétation et la chirurgie en présence de complications neurologiques sont des prédicteurs d’issue fatale dans l’analyse basée sur l’apprentissage automatique.
© 2021 The Authors.
Figures
References
-
- Habib G., Lancellotti P., Antunes Manuel J., et al. 2015 ESC guidelines for the management of infective endocarditis (ESC) Eur Heart J. 2015;36 3075-23. - PubMed
-
- Habib G., Erba B., Lung B., et al. Clinical presentation, aetiology and outcome of infective endocarditis. Results of the ESC-EORP EURO-ENDO (European infective endocarditis) registry: a prospective cohort study. Eur Heart J. 2019;40:3222–3233. - PubMed
-
- Fernandez-Hidalgo N., Almirante B., Tornos P., et al. Contemporary epidemiology and prognosis of health care–associated infective endocarditis. Clin Infect Dis. 2008;47:1287–1297. - PubMed
-
- Wang A., Gaca J., Chu V.H., et al. Management considerations in infective endocarditis: a review. JAMA. 2018;320:72–83. - PubMed
LinkOut - more resources
Full Text Sources
