

Anti-Müllerian hormone as a marker of ovarian reserve and premature ovarian insufficiency in children and women with cancer: a systematic review
- PMID: 35199161
- PMCID: PMC9071067
- DOI: 10.1093/humupd/dmac004
Anti-Müllerian hormone as a marker of ovarian reserve and premature ovarian insufficiency in children and women with cancer: a systematic review
Abstract
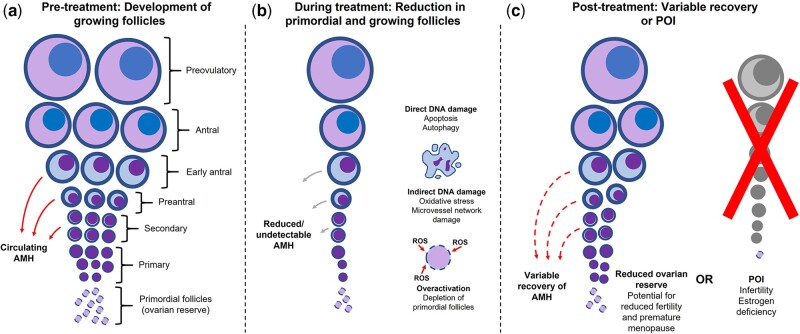
Background: Female patients undergoing anticancer treatment are at elevated risk of adverse ovarian outcomes including infertility and premature ovarian insufficiency (POI), which is associated with short- and long-term health risks. Anti-Müllerian hormone (AMH) is a key biomarker of ovarian reserve, but its role prior to and after cancer treatment is less well understood.
Objective and rationale: To conduct a systematic review evaluating AMH as a biomarker of ovarian reserve and POI before and after anticancer treatment, which has become a pressing clinical issue in reproductive medicine. There are a large number of observational studies, but differences in patient groups, cancer diagnoses and study design make this a confusing field that will benefit from a thorough and robust review.
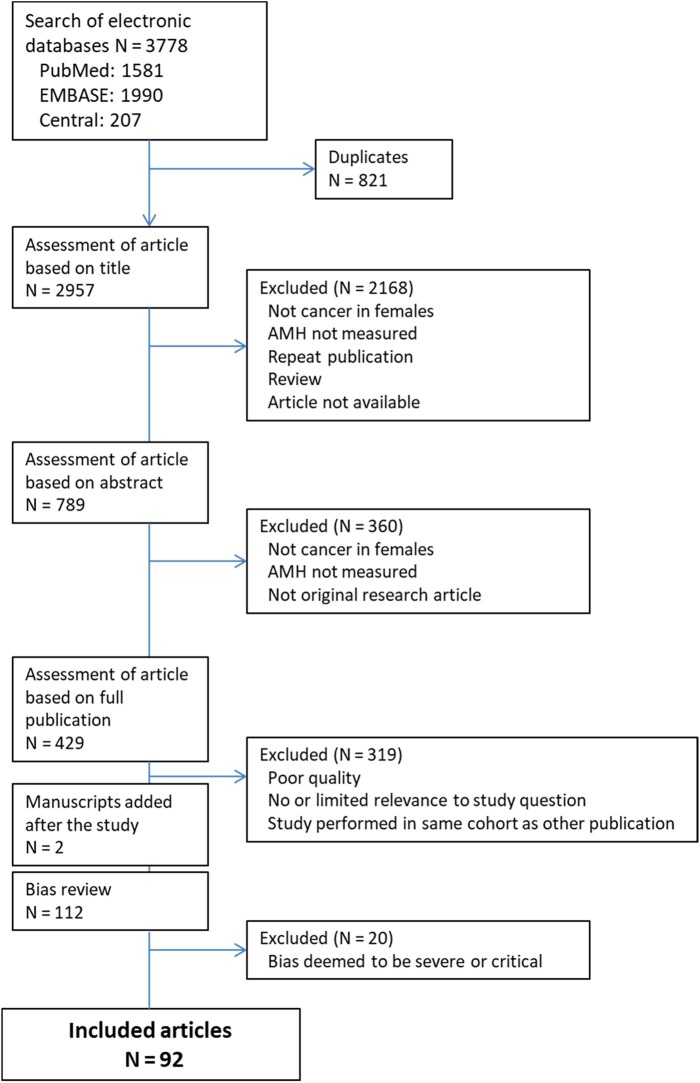
Search methods: A systematic literature search for AMH in women with cancer was conducted in PubMed, Embase and Cochrane Central Register of Controlled Trials up to 1 April 2021. Bias review was conducted using the Risk of Bias In Non-randomized Studies of Interventions (ROBINS-I) protocol along with qualitative assessment of quality. Exploratory subgroups were established based on age, cancer type and length of follow-up.
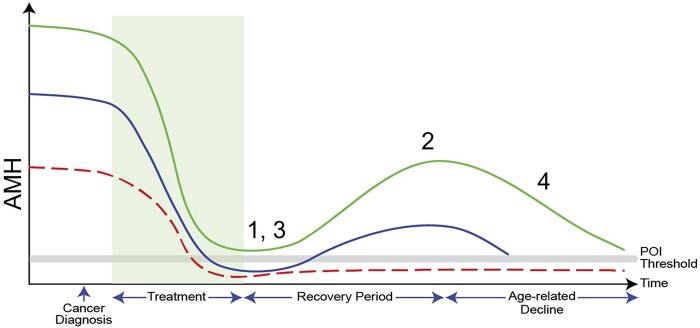
Outcomes: Ninety-two publications (N = 9183 patients) were included in this analysis after quality and bias review. Reduced/undetectable AMH was consistently identified in 69/75 studies (92%) following chemotherapy or radiotherapy, with reductions ranging from 42% to concentrations below the limit of detection, and many reporting mean or median declines of ≥90%. Where longitudinal data were analysed (42 studies), a majority (33/42 (79%)) of studies reported at least partial recovery of AMH at follow-up, however, effect estimates were highly variable, reflecting that AMH levels were strongly impacted by anticancer treatment (i.e. the chemotherapy regimen used and the number of treatment cycles need), with recovery and its degree determined by treatment regimen, age and pre-treatment AMH level. In 16/31 (52%) publications, oligo/amenorrhoea was associated with lower post-treatment AMH consistent with impending POI, although menstruation and/or pregnancy were reported in patients with low or undetectable AMH. Long-term (>5 years) follow-up of paediatric patients following cancer treatment also found significantly lower AMH compared with control groups in 14/20 (70%) of studies, with very variable effect sizes from complete loss of AMH to full recovery depending on treatment exposure, as in adult patients.
Wider implications: AMH can be used to identify the damaging effect of cancer treatments on ovarian function. This can be applied to individual women, including pre-pubertal and adolescent girls, as well as comparing different treatment regimens, ages and pre-treatment AMH levels in populations of women. While there was evidence for its value in the diagnosis of POI after cancer treatment, further studies across a range of diagnoses/treatment regimens and patient ages are required to clarify this, and to quantify its predictive value. A major limitation for the use of AMH clinically is the very limited data relating post-treatment AMH levels to fertility, duration of reproductive lifespan or time to POI; analysis of these clinically relevant outcomes will be important in further research.
Keywords: AMH; anti-Müllerian hormone; cancer; chemotherapy; fertility; gonadotoxicity; ovarian insufficiency; ovarian reserve.
© The Author(s) 2022. Published by Oxford University Press on behalf of European Society of Human Reproduction and Embryology.
Figures
References
-
- Acibucu F, Acibucu DO, Akkar OB, Dokmetas HS.. Evaluation of ovarian reserve with AMH level in patients with well-differentiated thyroid cancer receiving radioactive iodine ablation treatment. Exp Clin Endocrinol Diabetes 2016;124:593–596. - PubMed
-
- Al-Janabi HT, Al-Taee HA, Alawad AS.. The impact of age on antimullerian hormone serum level in women attending chemotherapy unit for primary breast cancer. Middle East Fertil Soc J 2018;23:126–130.
-
- Anderson RA, Cameron DA.. Pretreatment serum anti-mullerian hormone predicts long-term ovarian function and bone mass after chemotherapy for early breast cancer. J Clin Endocrinol Metab 2011;96:1336–1343. - PubMed
-
- Anderson RA, Remedios R, Kirkwood AA, Patrick P, Stevens L, Clifton-Hadley L, Roberts T, Hatton C, Kalakonda N, Milligan DW. et al. Determinants of ovarian function after response-adapted therapy in patients with advanced Hodgkin's lymphoma (RATHL): a secondary analysis of a randomised phase 3 trial. Lancet Oncol 2018;19:1328–1337. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
