

PMMA-Cement-PLIF Is Safe and Effective as a Single-Stage Posterior Procedure in Treating Pyogenic Erosive Lumbar Spondylodiscitis-A Single-Center Retrospective Study of 73 Cases
- PMID: 35200426
- PMCID: PMC8869766
- DOI: 10.3390/bioengineering9020073
PMMA-Cement-PLIF Is Safe and Effective as a Single-Stage Posterior Procedure in Treating Pyogenic Erosive Lumbar Spondylodiscitis-A Single-Center Retrospective Study of 73 Cases
Abstract
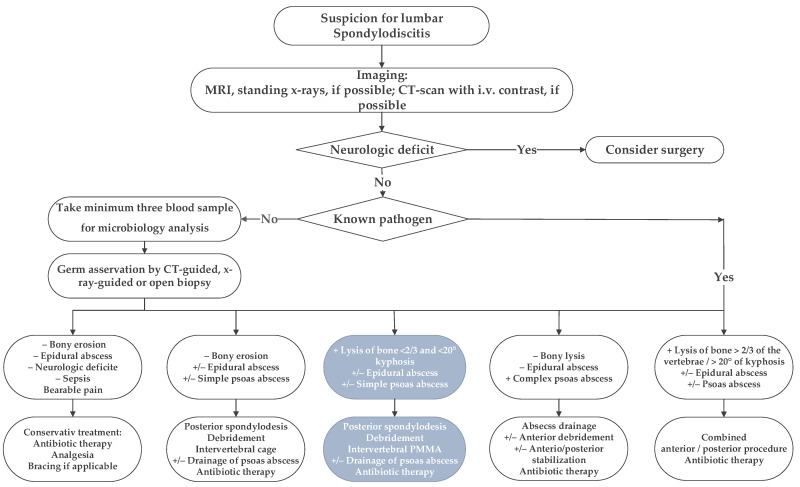
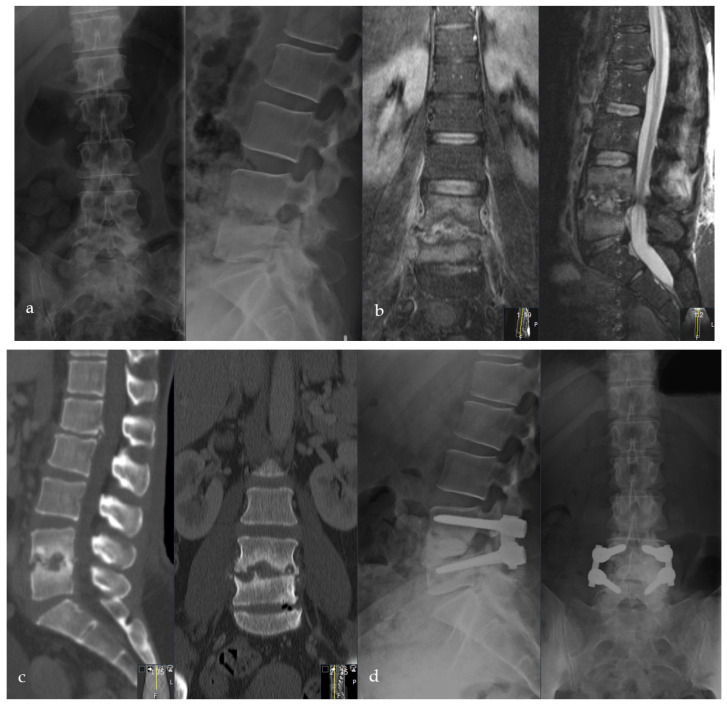
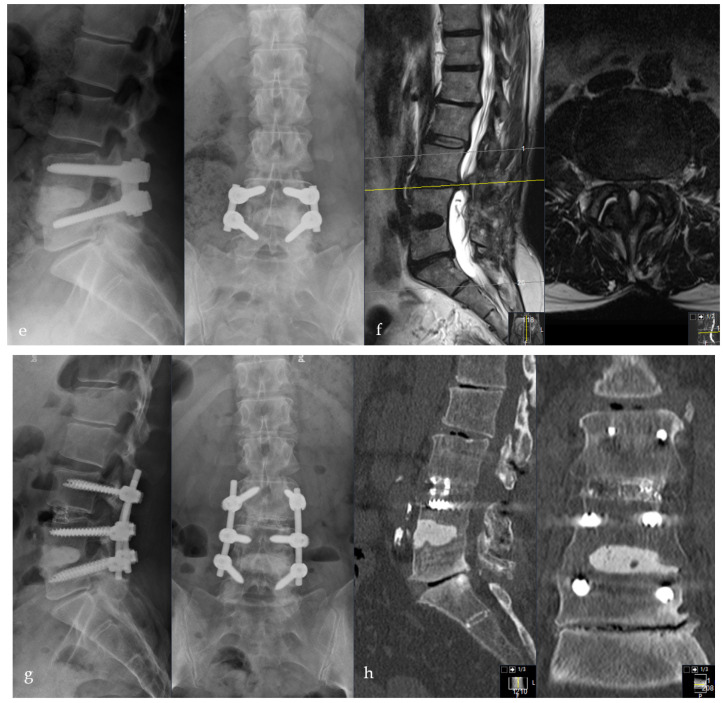
Background: Surgical treatment for erosive pyogenic spondylodiscitis of the lumbar spine is challenging as, following debridement of the intervertebral and bony abscess, a large and irregular defect is created. Sufficient defect reconstruction with conventional implants using a posterior approach is often impossible. Therefore, we developed the "Cement-PLIF", a single-stage posterior lumbar procedure, combining posterior lumbar interbody fusion (PLIF) with defect-filling using antibiotic-loaded polymethylmethacrylate (PMMA). This study first describes and evaluates the procedure's efficacy, safety, and infection eradication rate. Radiological implant stability, bone-regeneration, sagittal profile reconstruction, procedure-related complications, and pre-existing comorbidities were further analyzed.
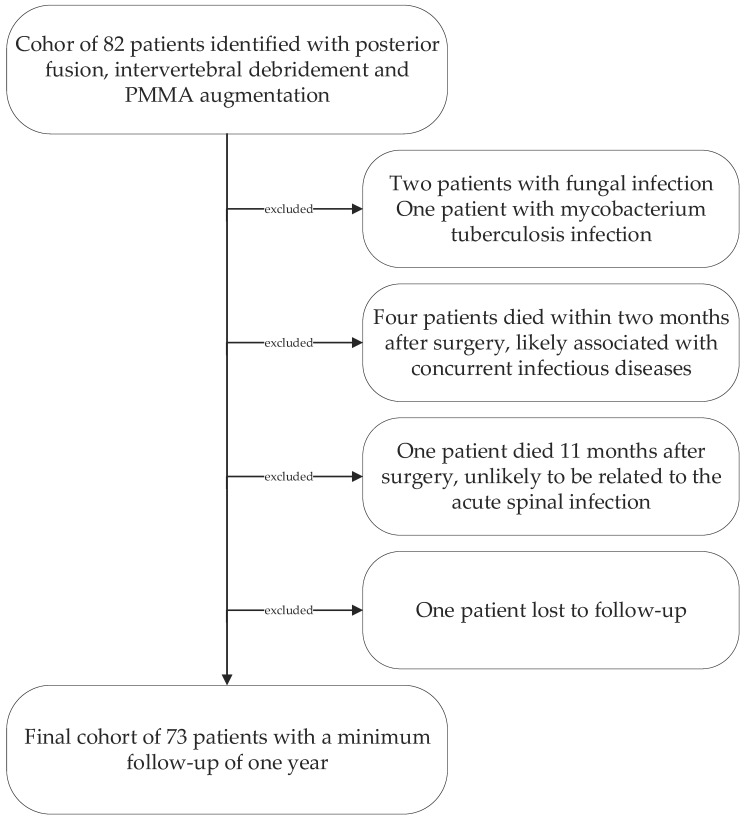
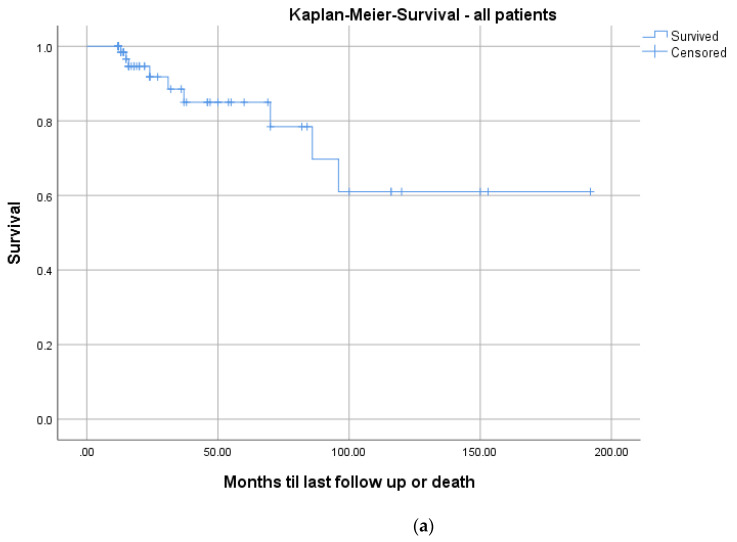
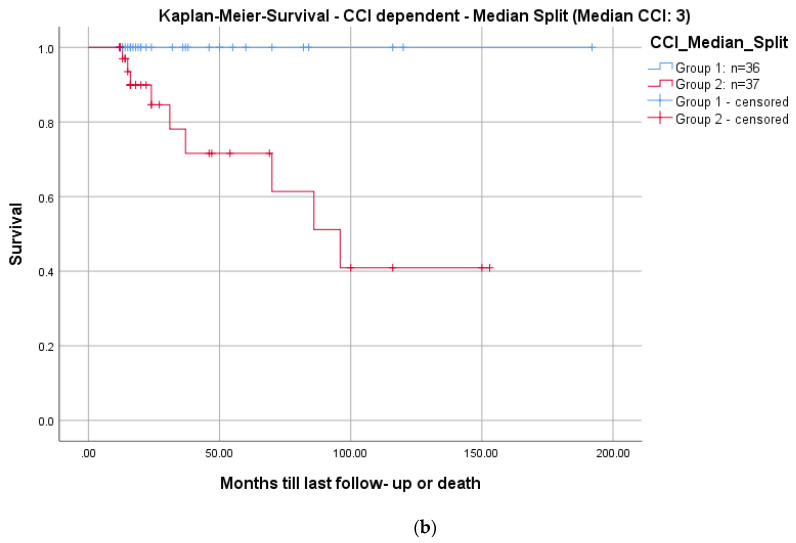
Methods: A retrospective cohort study analyzing 73 consecutive patients with a minimum of a one-year follow-up from 2000-2017. Patient-reported pain levels and improvement in infectious serological parameters evaluated the clinical outcome. Sagittal profile reconstruction, anterior bone-regeneration, and posterior fusion were analyzed in a.p. and lateral radiographs. A Kaplan-Meier analysis was used to determine the impact of pre-existing comorbidities on mortality. Pre-existing comorbidities were quantified using the Charlson-Comorbidity Index (CCI).
Results: Mean follow-up was 3.3 (range: 1-16; ±3.2) years. There was no evidence of infection persistence in all patients at the one-year follow-up. One patient underwent revision surgery for early local infection recurrence (1.4%). Five (6.9%) patients required an early secondary intervention at the same level due to minor complications. Radiological follow-up revealed implant stability in 70/73 (95.9%) cases. Successful sagittal reconstruction was demonstrated in all patients (p < 0.001). There was a significant correlation between Kaplan-Meier survival and the number of pre-existing comorbidities (24-months-survival: CCI ≤ 3: 100%; CCI ≥ 3: 84.6%; p = 0.005).
Conclusions: The Cement-PLIF procedure for pyogenic erosive spondylodiscitis is an effective and safe treatment as evaluated by infection elimination, clinical outcome, restoration, and maintenance of stability and sagittal alignment.
Keywords: PMMA; bony erosion; discitis; osteomyelitis; polymethylmethacrylate; spinal implants; spinal infection; spine; spondylodiscitis; staphylococcus aureus.
Conflict of interest statement
The authors declare no conflict of interest regarding the presented study.
Figures

Similar articles
-
One-stage Debridement via Oblique Lateral Interbody Fusion Corridor Combined with Posterior Pedicle Screw Fixation in Treating Spontaneous Lumbar Infectious Spondylodiscitis: A Case Series.Orthop Surg. 2019 Dec;11(6):1109-1119. doi: 10.1111/os.12562. Epub 2019 Nov 7. Orthop Surg. 2019. PMID: 31701667 Free PMC article.
-
Percutaneous Endoscopic Surgery Alone to Treat Severe Infectious Spondylodiscitis in the Thoracolumbar Spine: A Reparative Mechanism of Spontaneous Spinal Arthrodesis.Pain Physician. 2022 Mar;25(2):E299-E308. Pain Physician. 2022. PMID: 35322985
-
Single-level lumbar pyogenic spondylodiscitis treated with mini-open anterior debridement and fusion in combination with posterior percutaneous fixation via a modified anterior lumbar interbody fusion approach.J Neurosurg Spine. 2015 Dec;23(6):747-53. doi: 10.3171/2015.5.SPINE14876. Epub 2015 Sep 4. J Neurosurg Spine. 2015. PMID: 26340382
-
Clinical outcomes, safety, and cost considerations of rhBMP-2 in the surgical management of pyogenic spinal infections: a focused review.Eur Spine J. 2025 Jun 12. doi: 10.1007/s00586-025-08993-9. Online ahead of print. Eur Spine J. 2025. PMID: 40504240 Review.
-
Evaluation and Management of Pyogenic Spondylodiscitis: A Review.J Clin Med. 2025 May 15;14(10):3477. doi: 10.3390/jcm14103477. J Clin Med. 2025. PMID: 40429472 Free PMC article. Review.
Cited by
-
Surgical Treatment for Emphysematous Osteomyelitis of the Lumbar Spine: A Case Report.Spine Surg Relat Res. 2024 Apr 3;8(5):540-543. doi: 10.22603/ssrr.2024-0009. eCollection 2024 Sep 27. Spine Surg Relat Res. 2024. PMID: 39399456 Free PMC article. No abstract available.
-
Incidence and outcome of patients suffering from meningitis due to spondylodiscitis.Brain Spine. 2023 Aug 25;3:101781. doi: 10.1016/j.bas.2023.101781. eCollection 2023. Brain Spine. 2023. PMID: 38020984 Free PMC article.
-
Minimally Invasive versus Traditional Surgery: Efficacy of PELD and PLIF in Treating Pyogenic Spondylodiscitis.Med Sci Monit. 2024 Jul 19;30:e943176. doi: 10.12659/MSM.943176. Med Sci Monit. 2024. PMID: 39026435 Free PMC article.
-
Unilateral biportal endoscopic versus microscopic transforaminal lumbar interbody fusion for degenerative lumbar spinal stenosis in China: study protocol for a prospective, randomised, controlled, non-inferiority trial.BMJ Open. 2024 Sep 25;14(9):e083786. doi: 10.1136/bmjopen-2023-083786. BMJ Open. 2024. PMID: 39322595 Free PMC article.
-
PMMA-cement anterior column reconstruction in surgical treatment of spondylodiscitis.Brain Spine. 2022 Sep 17;2:101186. doi: 10.1016/j.bas.2022.101186. eCollection 2022. Brain Spine. 2022. PMID: 36248128 Free PMC article.
References
-
- Saeed K., Esposito S., Ascione T., Bassetti M., Bonnet E., Carnelutti A., Chan M., Lye D.C., Cortes N., Dryden M., et al. Hot topics on vertebral osteomyelitis from the International Society of Antimicrobial Chemotherapy. Int. J. Antimicrob. Agents. 2019;54:125–133. doi: 10.1016/j.ijantimicag.2019.06.013. - DOI - PubMed
-
- Tsiodras S., Falagas M.E. Clinical assessment and medical treatment of spine infections. Clin. Orthop. Relat. Res. 2006;444:38–50. doi: 10.1097/01.blo.0000203454.82264.cd. - DOI - PubMed
LinkOut - more resources
Full Text Sources
