

Cardiomyopathies in Children and Systemic Disorders When Is It Useful to Look beyond the Heart?
- PMID: 35200700
- PMCID: PMC8877723
- DOI: 10.3390/jcdd9020047
Cardiomyopathies in Children and Systemic Disorders When Is It Useful to Look beyond the Heart?
Abstract
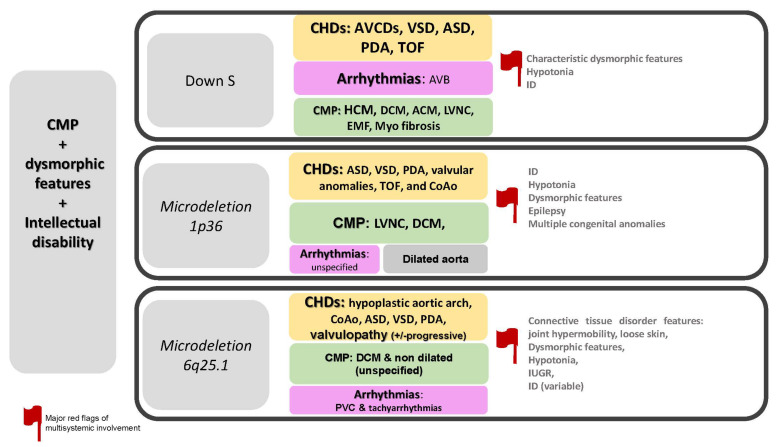
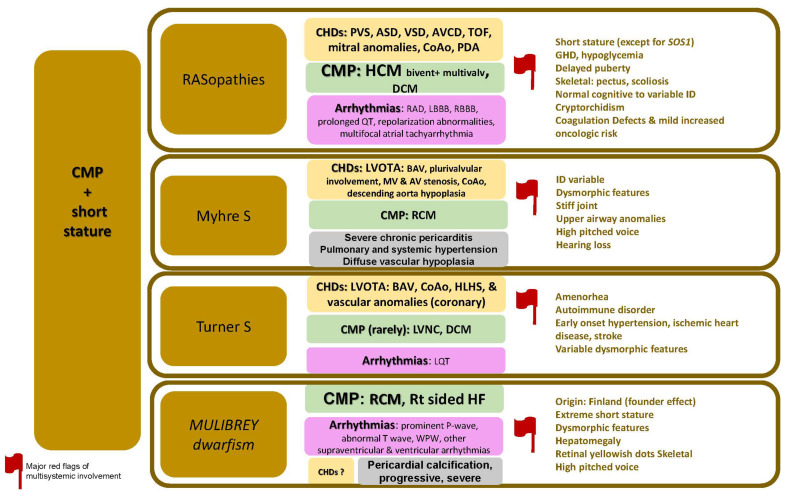
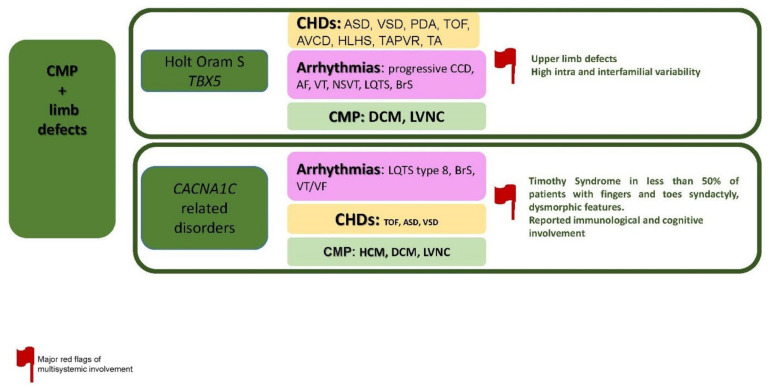
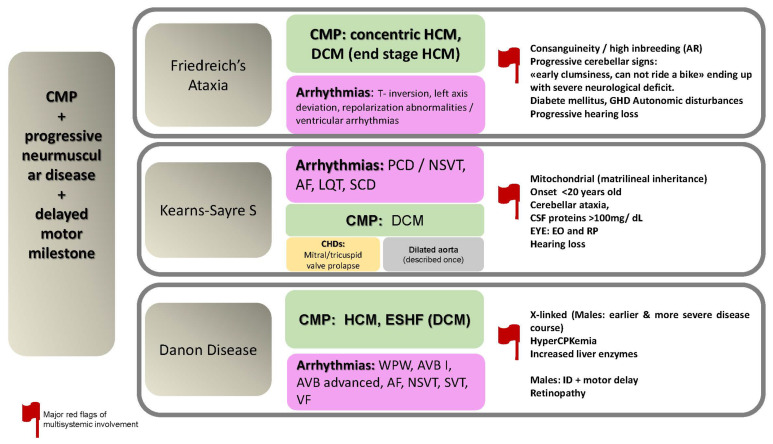
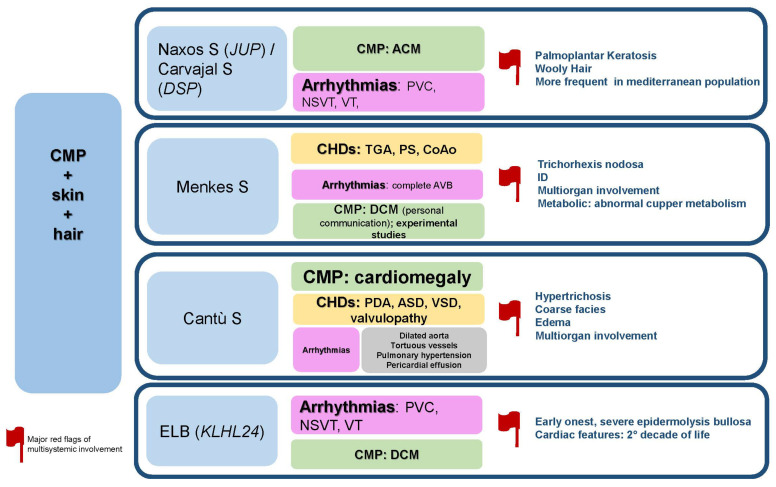
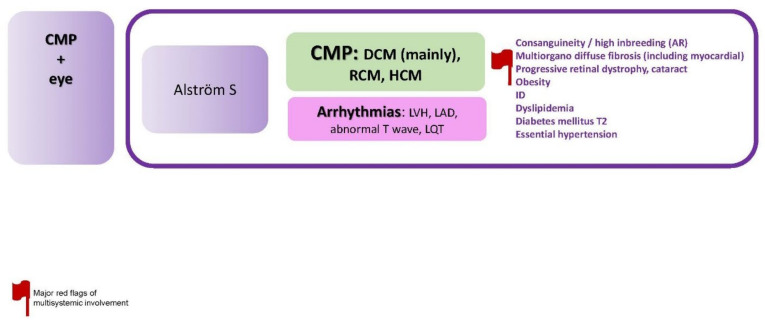
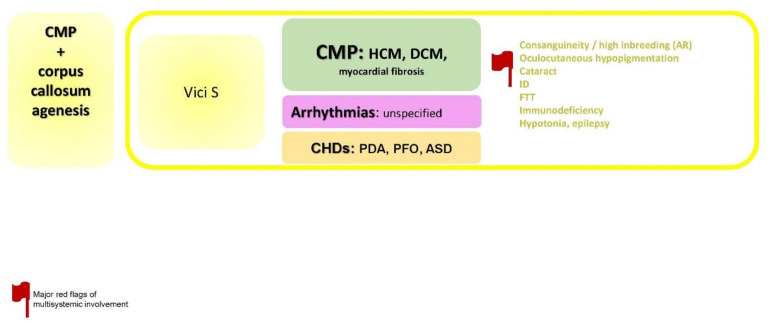
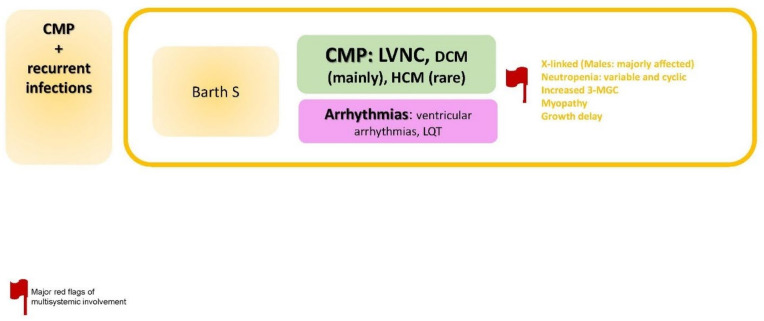
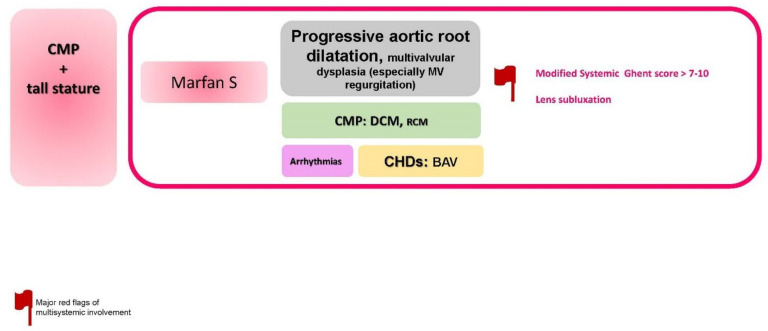
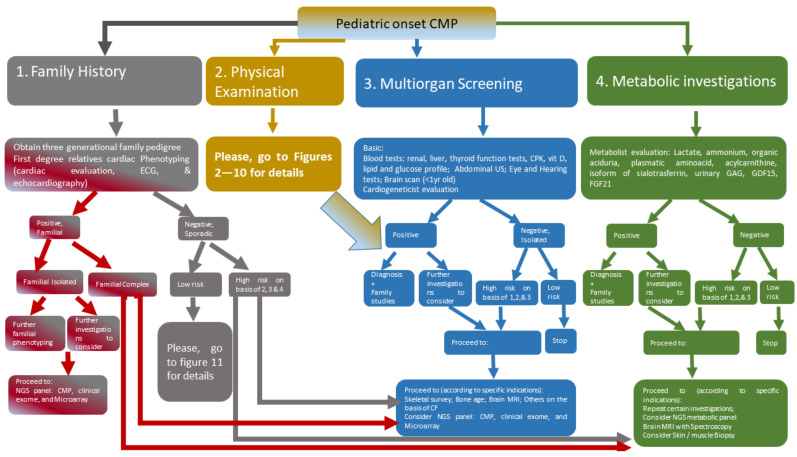
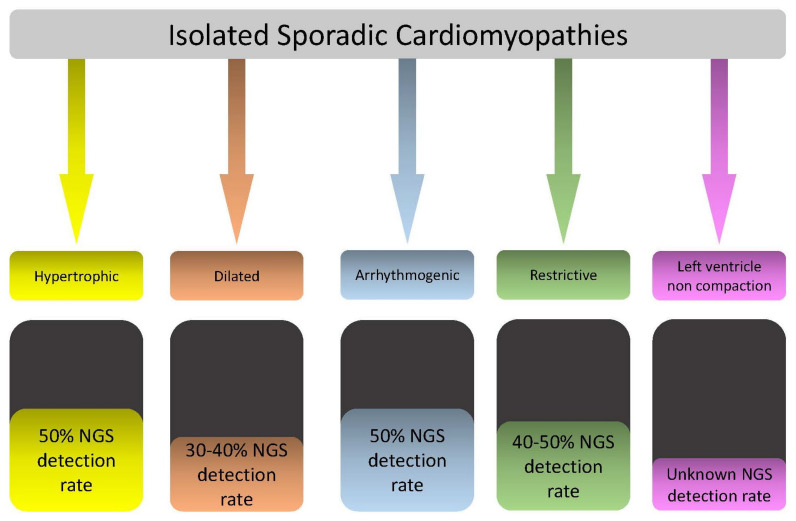
Cardiomyopathy (CMP) is a rare disease in the pediatric population, with a high risk of morbidity and mortality. The genetic etiology of CMPs in children is extremely heterogenous. These two factors play a major role in the difficulties of establishing standard diagnostic and therapeutic protocols. Isolated CMP in children is a frequent finding, mainly caused by sarcomeric gene variants with a detection rate that can reach up to 50% of analyzed cohorts. Complex multisystemic forms of pediatric CMP are even more heterogenous. Few studies in literature take into consideration this topic as the main core since it represents a rarity (systemic CMP) within a rarity (pediatric population CMP). Identifying etiology in this cohort is essential for understanding prognosis, risk stratification, eligibility to heart transplantation and/or mechanical-assisted procedures, preventing multiorgan complications, and relatives' recurrence risk calculation. The previous points represent a cornerstone in patients' empowerment and personalized medical care approach. The aim of this work is to propose a new approach for an algorithm in the setting of the diagnostic framework of systemic pediatric CMP. On the other hand, during the literature review, we noticed a relatively common etiologic pattern in some forms of complex/multisystem CMP. In other words, certain syndromes such as Danon, Vici, Alström, Barth, and Myhre syndrome share a common pathway of directly or indirectly defective "autophagy" process, which appears to be a possible initiating/triggering factor for CMPs. This conjoint aspect could be important for possible prognostic/therapeutic implications in this category of patients. However, multicentric studies detailed functional and experimental models are needed prior to deriving conclusions.
Keywords: cardiomyopathies; children; heterogeneity; multisystemic; personalized approach; syndromes.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Andrews R.E., Fenton M.J., Ridout D.A., Burch M., British Congenital Cardiac Association New-Onset Heart Failure Due to Heart Muscle Disease in Childhood: A Prospective Study in the United Kingdom and Ireland: A Prospective Study in the United Kingdom and Ireland. Circulation. 2008;117:79–84. doi: 10.1161/CIRCULATIONAHA.106.671735. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
