

Multimodality Imaging in Ischemic Chronic Cardiomyopathy
- PMID: 35200737
- PMCID: PMC8877428
- DOI: 10.3390/jimaging8020035
Multimodality Imaging in Ischemic Chronic Cardiomyopathy
Abstract
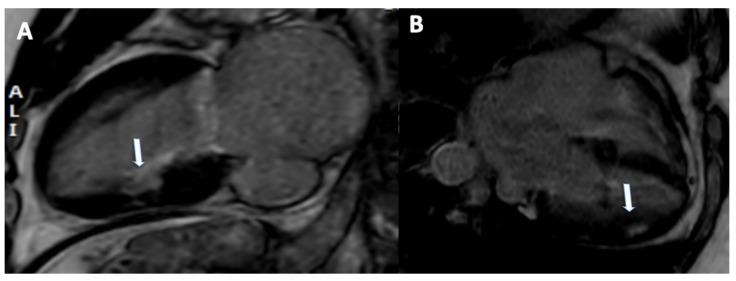
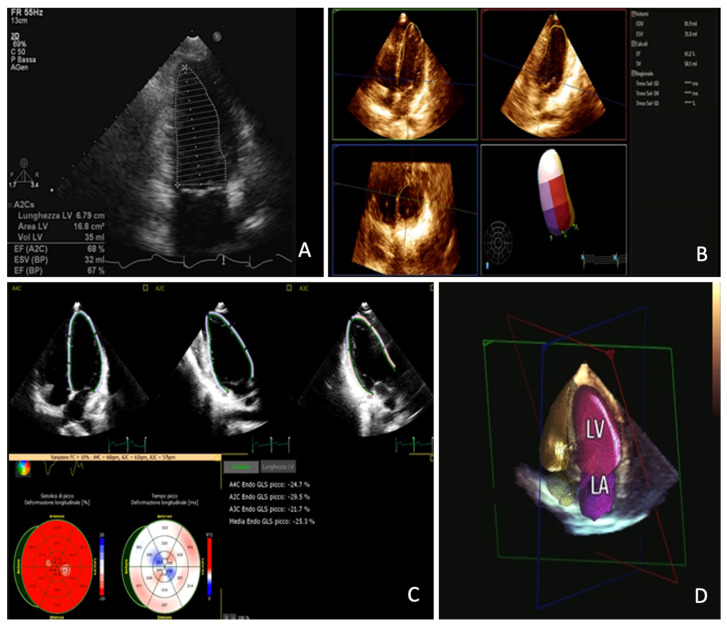
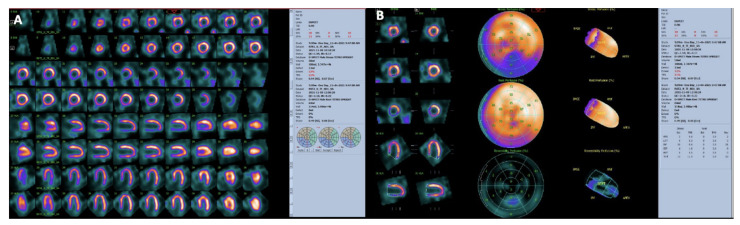
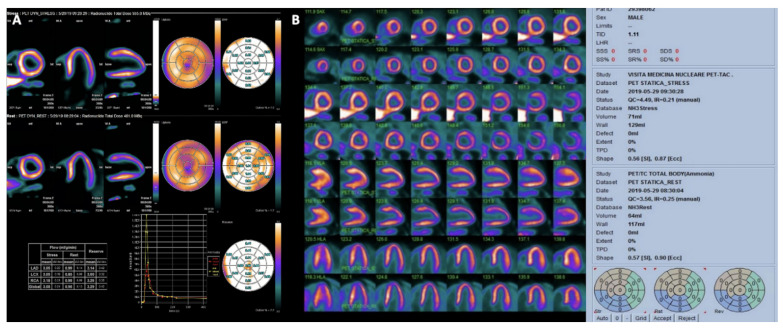
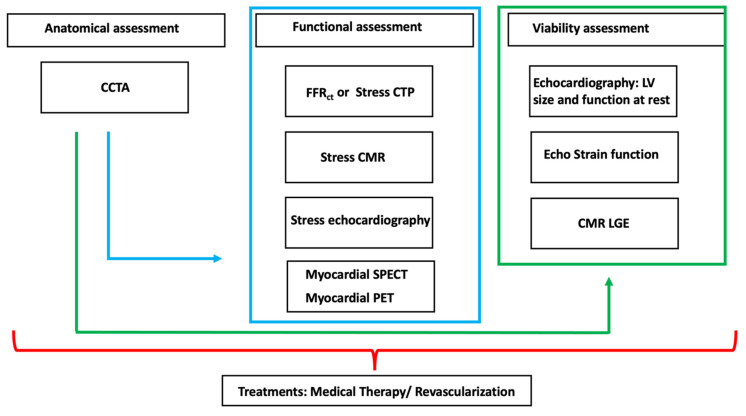
Ischemic chronic cardiomyopathy (ICC) is still one of the most common cardiac diseases leading to the development of myocardial ischemia, infarction, or heart failure. The application of several imaging modalities can provide information regarding coronary anatomy, coronary artery disease, myocardial ischemia and tissue characterization. In particular, coronary computed tomography angiography (CCTA) can provide information regarding coronary plaque stenosis, its composition, and the possible evaluation of myocardial ischemia using fractional flow reserve CT or CT perfusion. Cardiac magnetic resonance (CMR) can be used to evaluate cardiac function as well as the presence of ischemia. In addition, CMR can be used to characterize the myocardial tissue of hibernated or infarcted myocardium. Echocardiography is the most widely used technique to achieve information regarding function and myocardial wall motion abnormalities during myocardial ischemia. Nuclear medicine can be used to evaluate perfusion in both qualitative and quantitative assessment. In this review we aim to provide an overview regarding the different noninvasive imaging techniques for the evaluation of ICC, providing information ranging from the anatomical assessment of coronary artery arteries to the assessment of ischemic myocardium and myocardial infarction. In particular this review is going to show the different noninvasive approaches based on the specific clinical history of patients with ICC.
Keywords: cardiac magnetic resonance; chronic ischemic cardiomyopathy; computed tomography angiography; echocardiography; multimodality imaging; nuclear medicine.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Muscogiuri G., Ricci F., Scafuri S., Guglielmo M., Baggiano A., De Stasio V., Di Donna C., Spiritigliozzi L., Chiocchi M., Lee S.J., et al. Cardiac Magnetic Resonance Tissue Characterization in Ischemic Cardiomyopathy. J. Thorac. Imaging. 2021;37:2–16. doi: 10.1097/RTI.0000000000000621. - DOI - PubMed
-
- Kadoglou N.P.E., Papadopoulos C.H., Papadopoulos K.G., Karagiannis S., Karabinos I., Loizos S., Theodosis-Georgilas A., Aggeli K., Keramida K., Klettas D., et al. Updated knowledge and practical implementations of stress echocardiography in ischemic and non-ischemic cardiac diseases: An expert consensus of the Working Group of Echocardiography of the Hellenic Society of Cardiology. Hellenic J. Cardiol. 2021 doi: 10.1016/j.hjc.2021.07.006. In Press . - DOI - PubMed
