

Minimizing treatment-induced emergence of antibiotic resistance in bacterial infections
- PMID: 35201862
- PMCID: PMC7612469
- DOI: 10.1126/science.abg9868
Minimizing treatment-induced emergence of antibiotic resistance in bacterial infections
Abstract
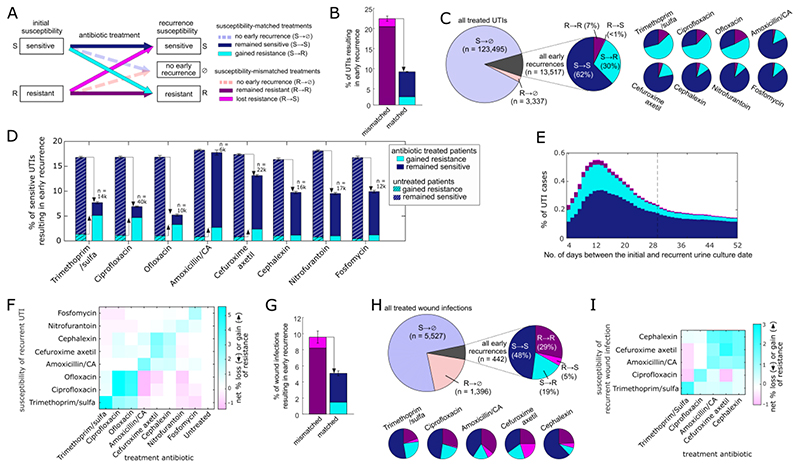
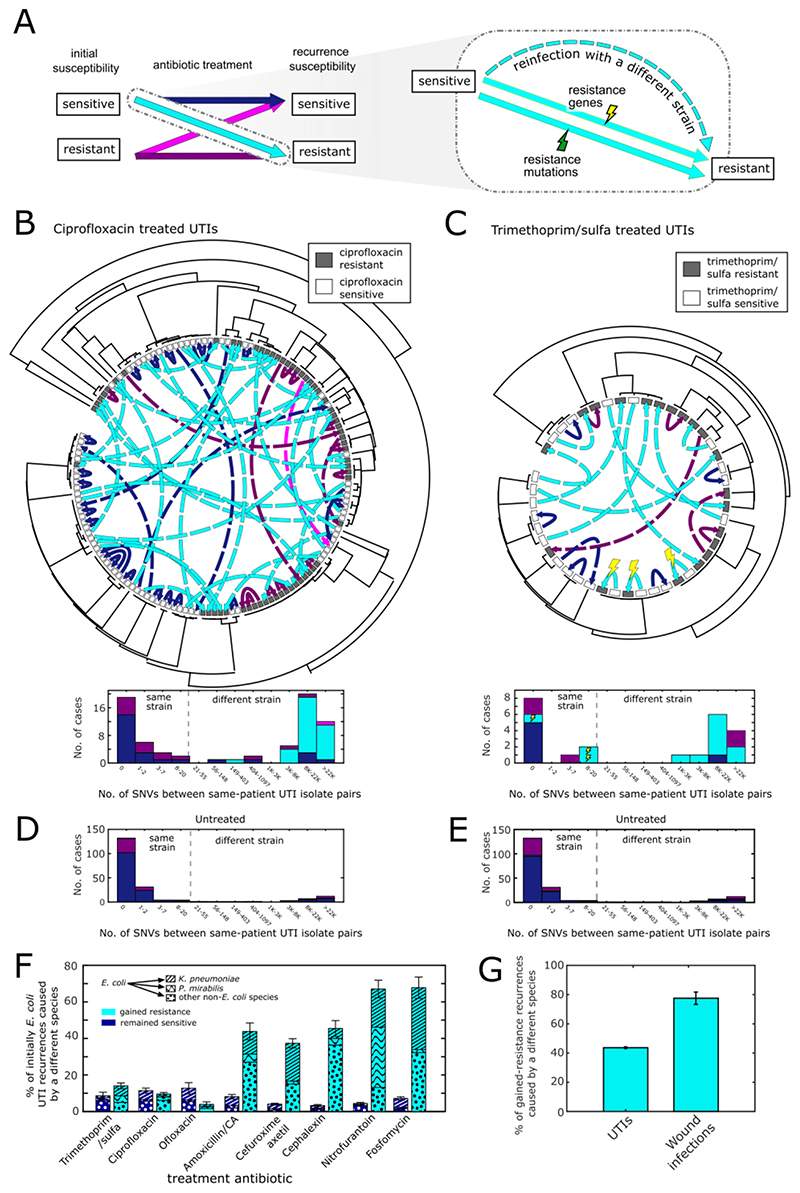
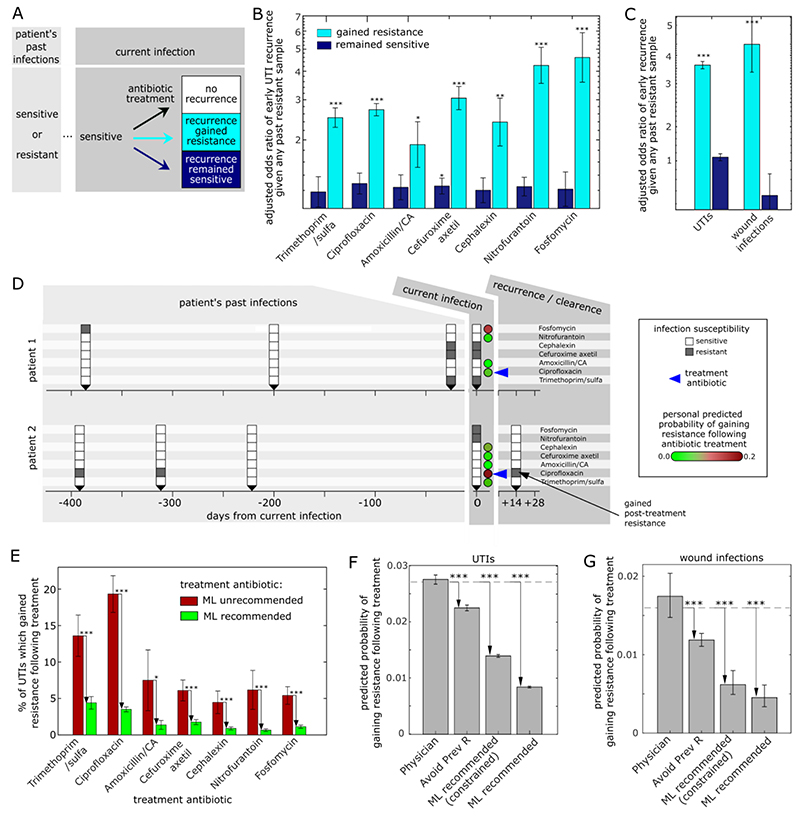
Treatment of bacterial infections currently focuses on choosing an antibiotic that matches a pathogen's susceptibility, with less attention paid to the risk that even susceptibility-matched treatments can fail as a result of resistance emerging in response to treatment. Combining whole-genome sequencing of 1113 pre- and posttreatment bacterial isolates with machine-learning analysis of 140,349 urinary tract infections and 7365 wound infections, we found that treatment-induced emergence of resistance could be predicted and minimized at the individual-patient level. Emergence of resistance was common and driven not by de novo resistance evolution but by rapid reinfection with a different strain resistant to the prescribed antibiotic. As most infections are seeded from a patient's own microbiota, these resistance-gaining recurrences can be predicted using the patient's past infection history and minimized by machine learning-personalized antibiotic recommendations, offering a means to reduce the emergence and spread of resistant pathogens.
Conflict of interest statement
Authors declare that they have no competing interests.
Figures
Comment in
-
Anticipating antibiotic resistance.Science. 2022 Feb 25;375(6583):818-819. doi: 10.1126/science.abn9969. Epub 2022 Feb 24. Science. 2022. PMID: 35201873
-
Machine-learning approaches prevent post-treatment resistance-gaining bacterial recurrences.Trends Microbiol. 2022 Jul;30(7):612-614. doi: 10.1016/j.tim.2022.05.006. Epub 2022 May 19. Trends Microbiol. 2022. PMID: 35599112
-
Infection and Inflammation of the Genitourinary Tract.J Urol. 2022 Nov;208(5):1141-1142. doi: 10.1097/JU.0000000000002906. Epub 2022 Aug 11. J Urol. 2022. PMID: 35950377 No abstract available.
-
Urolithiasis/Endourology.J Urol. 2022 Nov;208(5):1154-1155. doi: 10.1097/JU.0000000000002913. Epub 2022 Aug 17. J Urol. 2022. PMID: 35975568 No abstract available.
-
Uro-Science.J Urol. 2022 Nov;208(5):1152-1153. doi: 10.1097/JU.0000000000002932. Epub 2022 Aug 22. J Urol. 2022. PMID: 35993121 No abstract available.
References
-
- Harding GKM, Ronald AR. The management of urinary infections; what have we learned in the past decade? Int J Antimicrob Agents. 1994;4:83–88. - PubMed
-
- Stamm WE, Norrby SR. Urinary tract infections: disease panorama and challenges. J Infect Dis. 2001;183(Suppl 1):S1–4. - PubMed
-
- Nicolle Lindsay E. Brenner and Rector’s The Kidney. 10th Editi. Elsevier; 2015. pp. 1231–1256.
-
- Tchesnokova VL, Rechkina E, Chan D, Haile HG, Larson L, Ferrier K, Schroeder DW, Solyanik T, Shibuya S, Hansen K, Ralston JD, et al. Pandemic Uropathogenic Fluoroquinolone-resistant Escherichia coli Have Enhanced Ability to Persist in the Gut and Cause Bacteriuria in Healthy Women. Clinical Infectious Diseases. 2019 doi: 10.1093/cid/ciz547. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
