

COVID-19 Pneumonia and Lung Cancer: A Challenge for the RadiologistReview of the Main Radiological Features, Differential Diagnosis and Overlapping Pathologies
- PMID: 35202206
- PMCID: PMC8875889
- DOI: 10.3390/tomography8010041
COVID-19 Pneumonia and Lung Cancer: A Challenge for the RadiologistReview of the Main Radiological Features, Differential Diagnosis and Overlapping Pathologies
Abstract
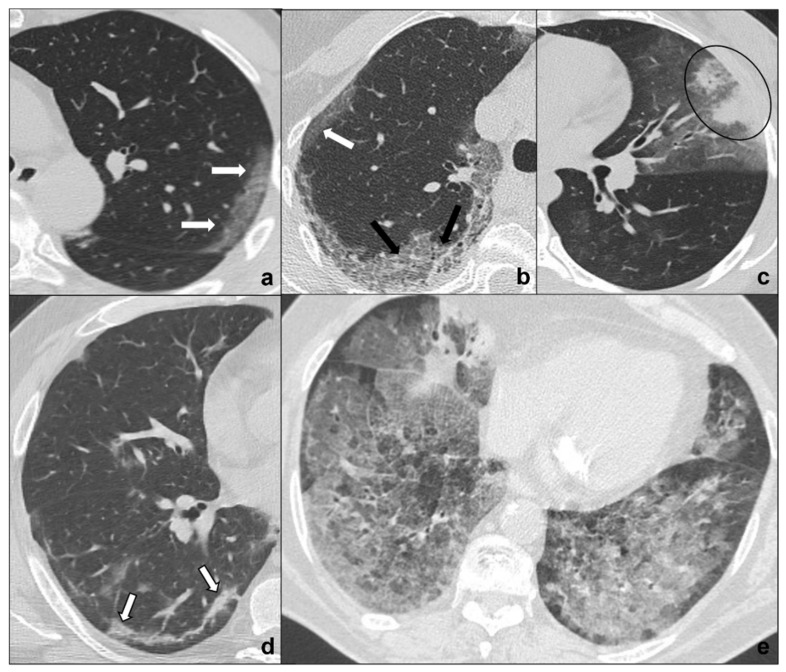
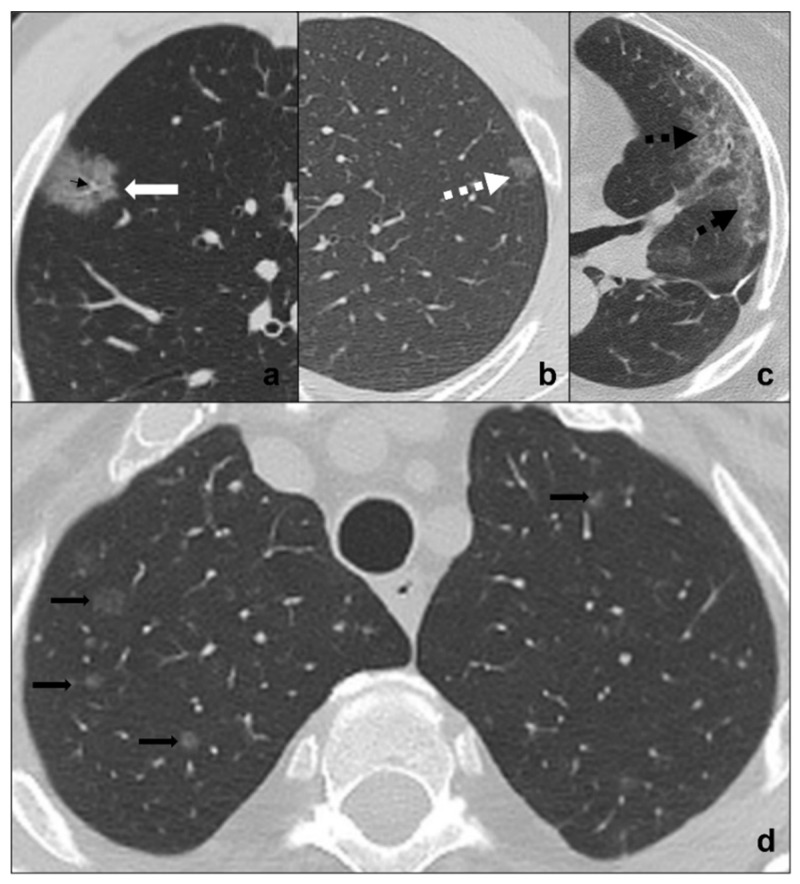
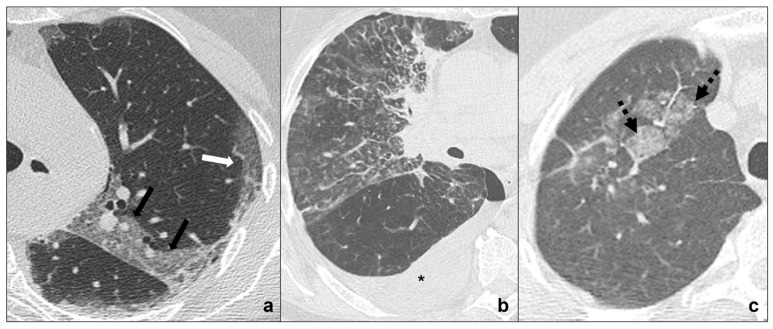
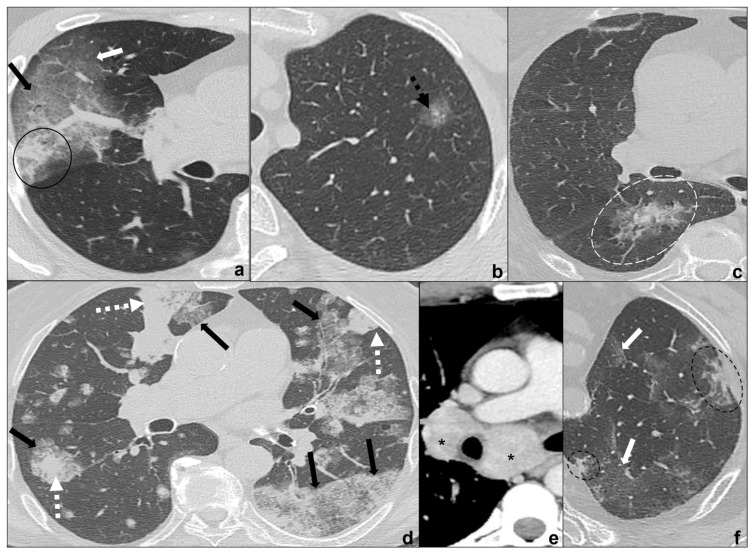
The COVID-19 pneumonia pandemic represents the most severe health emergency of the 21st century and has been monopolizing health systems' economic and human resources world-wide. Cancer patients have been suffering from the health systems' COVID-19 priority management with evidence of late diagnosis leading to patients' poor prognosis and late medical treatment. The radiologist plays a pivotal role as CT represents a non-invasive radiological technique which may help to identify possible overlap and differential diagnosis between COVID-19 pneumonia and lung cancer, which represents the most frequent cancer histology in COVID-19 patients. Our aims are: to present the main CT features of COVID-19 pneumonia; to provide the main differential diagnosis with lung cancer, chemotherapy-, immunotherapy-, and radiotherapy-induced lung disease; and to suggest practical tips and key radiological elements to identify possible overlap between COVID-19 pneumonia and lung cancer. Despite similarities or overlapping findings, the combination of clinics and some specific radiological findings, which are also identified by comparison with previous and follow-up CT scans, may guide differential diagnosis. It is crucial to search for typical COVID-19 pneumonia phase progression and typical radiological features on HRTC. The evidence of atypical findings such as lymphadenopathies and mediastinal and vessel invasion, as well as the absence of response to therapy, should arouse the suspicion of lung cancer and require contrast administration. Ground-glass areas and/or consolidations bound to radiotherapy fields or pneumonitis arising during and after oncological therapy should always arouse the suspicion of radiation-induced lung disease and chemo/immunotherapy-induced lung disease. The radiological elements we suggest for COVID-19 and lung cancer differential diagnosis may be used to develop AI protocols to guarantee an early and proper diagnosis and treatment to improve patients' quality of life and life expectancy.
Keywords: 2021; COVID-19; SARS-CoV-2; WHO; artificial intelligence; cancer; crazy paving; ground glass; lung cancer; omicron; pneumonia; variants.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Idiopathic Interstitial Pneumonias and COVID-19 Pneumonia: Review of the Main Radiological Features and Differential Diagnosis.Tomography. 2021 Aug 31;7(3):397-411. doi: 10.3390/tomography7030035. Tomography. 2021. PMID: 34564297 Free PMC article. Review.
-
Challenges in the Differential Diagnosis of COVID-19 Pneumonia: A Pictorial Review.Diagnostics (Basel). 2022 Nov 16;12(11):2823. doi: 10.3390/diagnostics12112823. Diagnostics (Basel). 2022. PMID: 36428883 Free PMC article. Review.
-
Differential diagnoses of COVID-19 pneumonia: the current challenge for the radiologist-a pictorial essay.Insights Imaging. 2021 Mar 11;12(1):34. doi: 10.1186/s13244-021-00967-x. Insights Imaging. 2021. PMID: 33704615 Free PMC article. Review.
-
COVIDiag: a clinical CAD system to diagnose COVID-19 pneumonia based on CT findings.Eur Radiol. 2021 Jan;31(1):121-130. doi: 10.1007/s00330-020-07087-y. Epub 2020 Aug 1. Eur Radiol. 2021. PMID: 32740817 Free PMC article.
-
Differential Diagnosis of COVID-19 Pneumonia in Cancer Patients Received Radiotherapy.Int J Med Sci. 2020 Sep 16;17(16):2561-2569. doi: 10.7150/ijms.46133. eCollection 2020. Int J Med Sci. 2020. PMID: 33029098 Free PMC article.
Cited by
-
Habitat Imaging Biomarkers for Diagnosis and Prognosis in Cancer Patients Infected with COVID-19.Cancers (Basel). 2022 Dec 31;15(1):275. doi: 10.3390/cancers15010275. Cancers (Basel). 2022. PMID: 36612278 Free PMC article.
-
Prognostic Factors and Outcomes in Advanced Stage Lung Cancer Patients with COVID-19 Omicron Variant Infection.Int J Gen Med. 2023 Dec 15;16:5947-5953. doi: 10.2147/IJGM.S436917. eCollection 2023. Int J Gen Med. 2023. PMID: 38115968 Free PMC article.
-
Dynamic change of COVID-19 lung infection evaluated using co-registration of serial chest CT images.Front Public Health. 2022 Aug 12;10:915615. doi: 10.3389/fpubh.2022.915615. eCollection 2022. Front Public Health. 2022. PMID: 36033815 Free PMC article.
-
A Thorough Review of the Clinical Applications of Artificial Intelligence in Lung Cancer.Cancers (Basel). 2025 Mar 4;17(5):882. doi: 10.3390/cancers17050882. Cancers (Basel). 2025. PMID: 40075729 Free PMC article. Review.
-
A non-enhanced CT-based deep learning diagnostic system for COVID-19 infection at high risk among lung cancer patients.Front Med (Lausanne). 2024 Aug 12;11:1444708. doi: 10.3389/fmed.2024.1444708. eCollection 2024. Front Med (Lausanne). 2024. PMID: 39188873 Free PMC article.
References
-
- Chan J.F.-W., Yuan S., Kok K.-H., To K.K.-W., Chu H., Yang J., Xing F., Liu J., Yip C.C.-Y., Poon R.W.-S., et al. A Familial Cluster of Pneumonia Associated with the 2019 Novel Coronavirus Indicating Person-to-Person Transmission: A Study of a Family Cluster. Lancet. 2020;395:514–523. doi: 10.1016/S0140-6736(20)30154-9. - DOI - PMC - PubMed
-
- Tracking SARS-CoV-2 Variants. [(accessed on 25 December 2021)]. Available online: https://www.who.int/activities/tracking-SARS-CoV-2-variants.
-
- Classification of Omicron (B.1.1.529): SARS-CoV-2 Variant of Concern. [(accessed on 25 December 2021)]. Available online: https://www.who.int/news/item/26-11-2021-classification-of-omicron-(b.1.....
-
- Talic S., Shah S., Wild H., Gasevic D., Maharaj A., Ademi Z., Li X., Xu W., Mesa-Eguiagaray I., Rostron J., et al. Effectiveness of Public Health Measures in Reducing the Incidence of COVID-19, SARS-CoV-2 Transmission, and COVID-19 Mortality: Systematic Review and Meta-Analysis. BMJ. 2021;375:e068302. - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
