

Stable Gastric Pentadecapeptide BPC 157 May Counteract Myocardial Infarction Induced by Isoprenaline in Rats
- PMID: 35203478
- PMCID: PMC8869603
- DOI: 10.3390/biomedicines10020265
Stable Gastric Pentadecapeptide BPC 157 May Counteract Myocardial Infarction Induced by Isoprenaline in Rats
Abstract
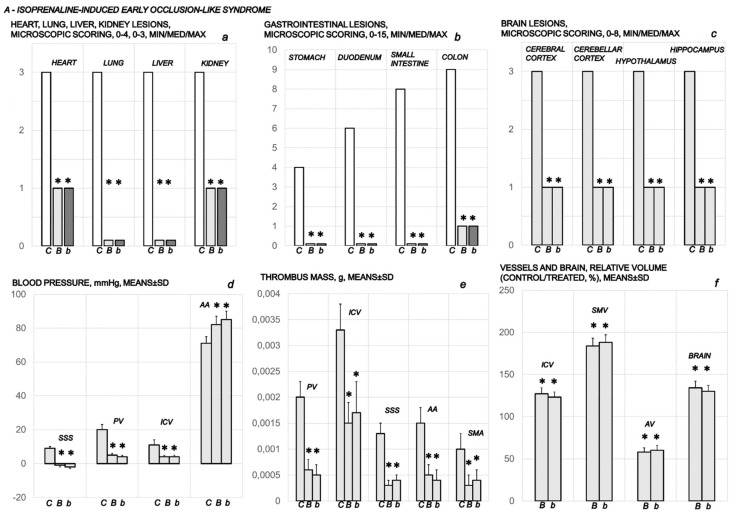
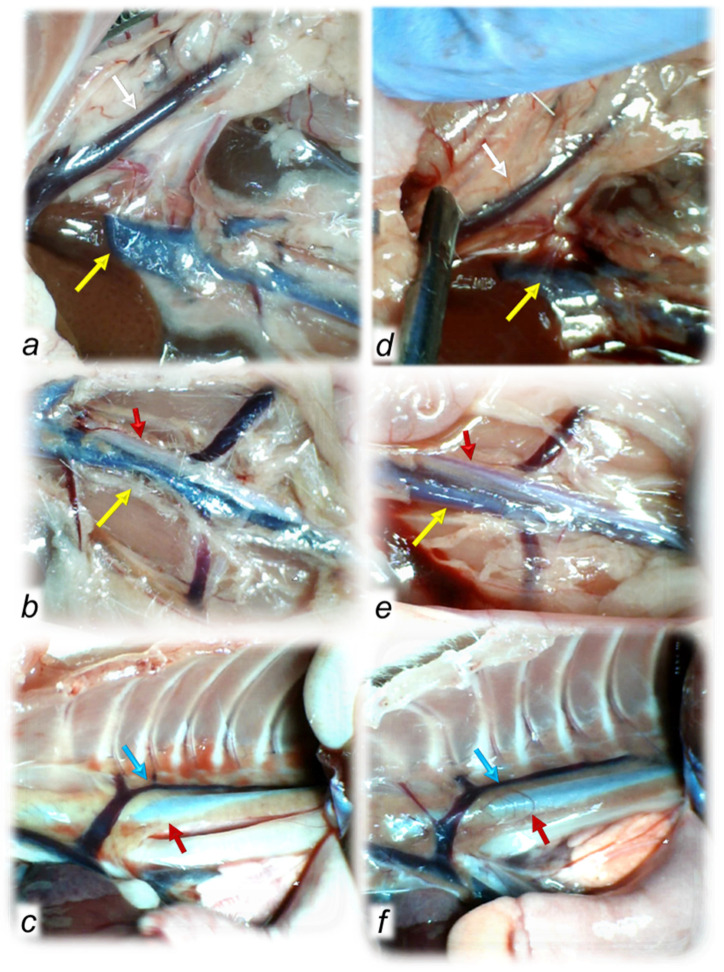
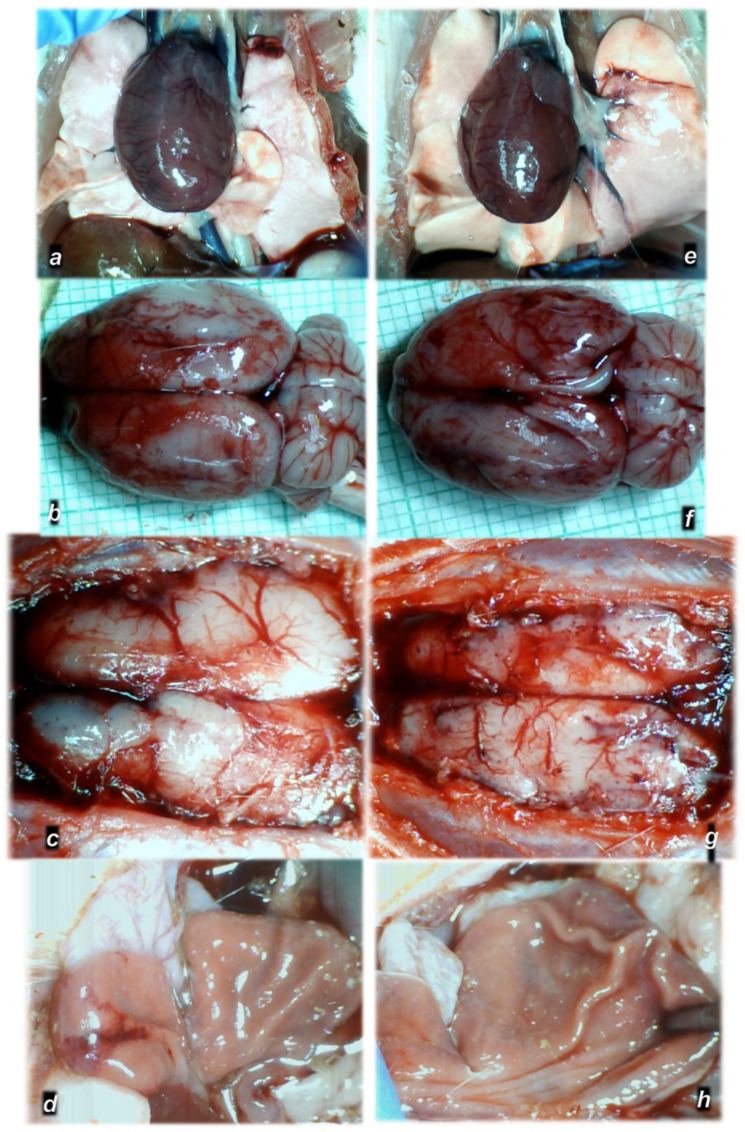
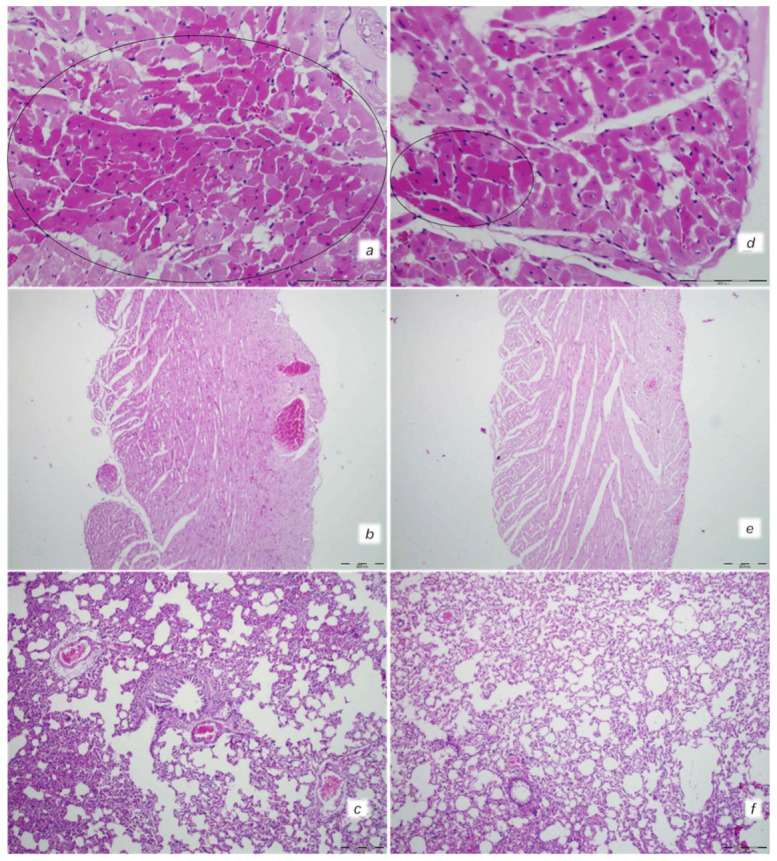
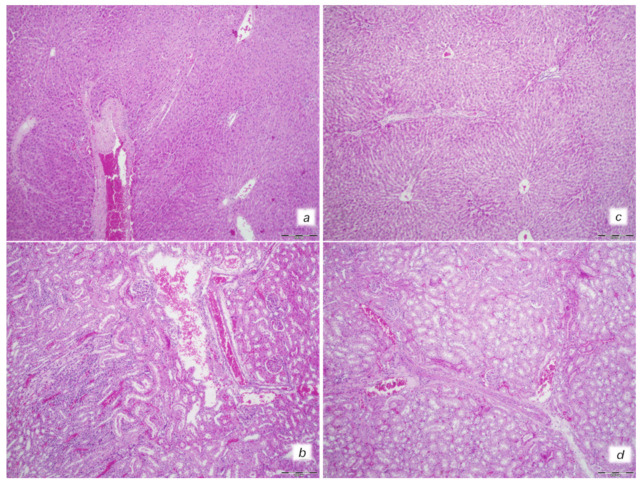
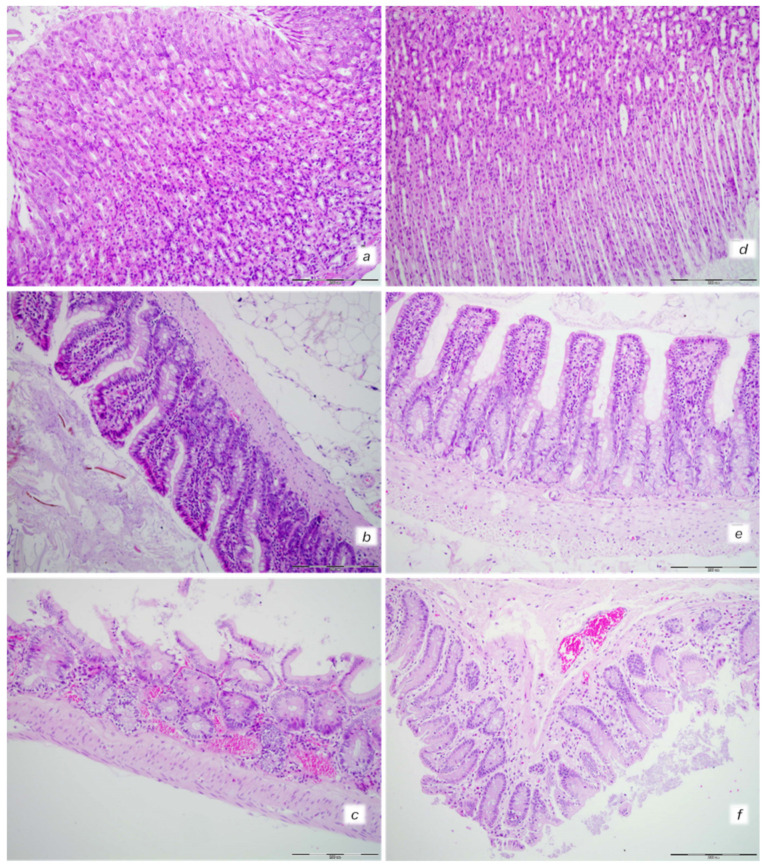
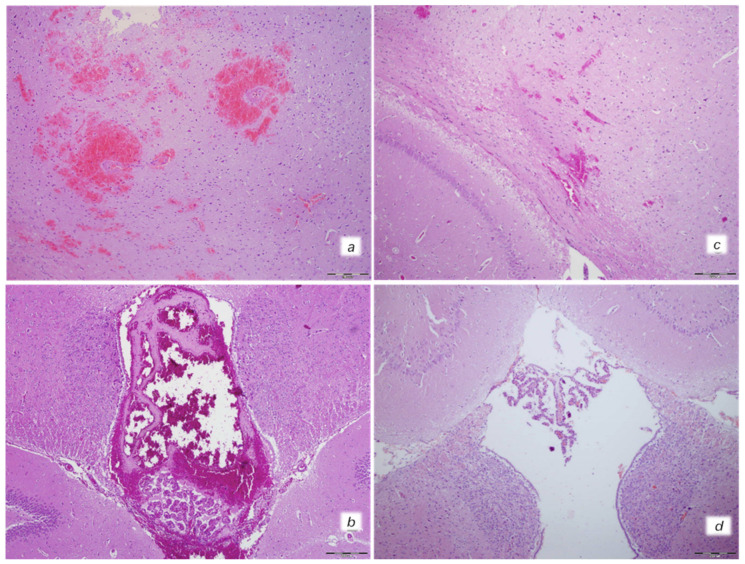
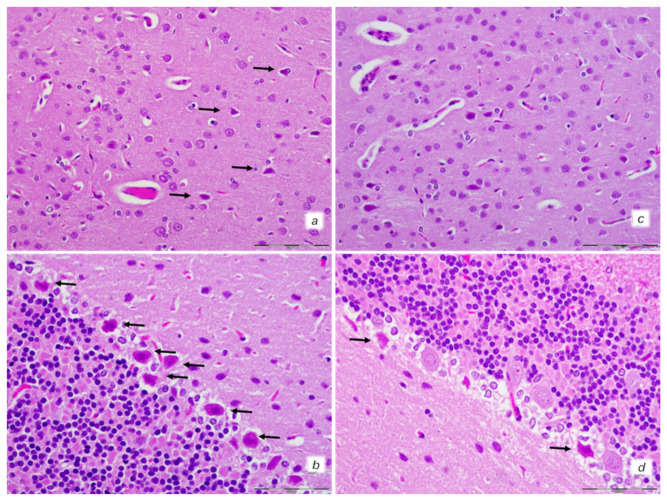
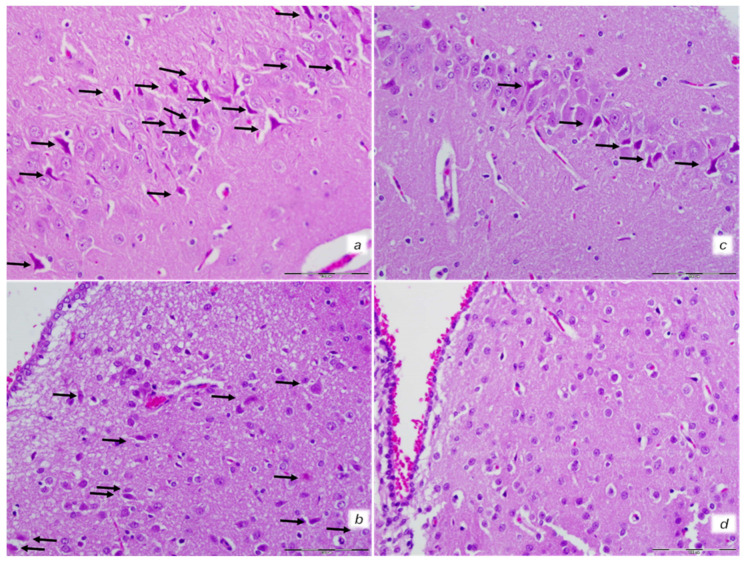
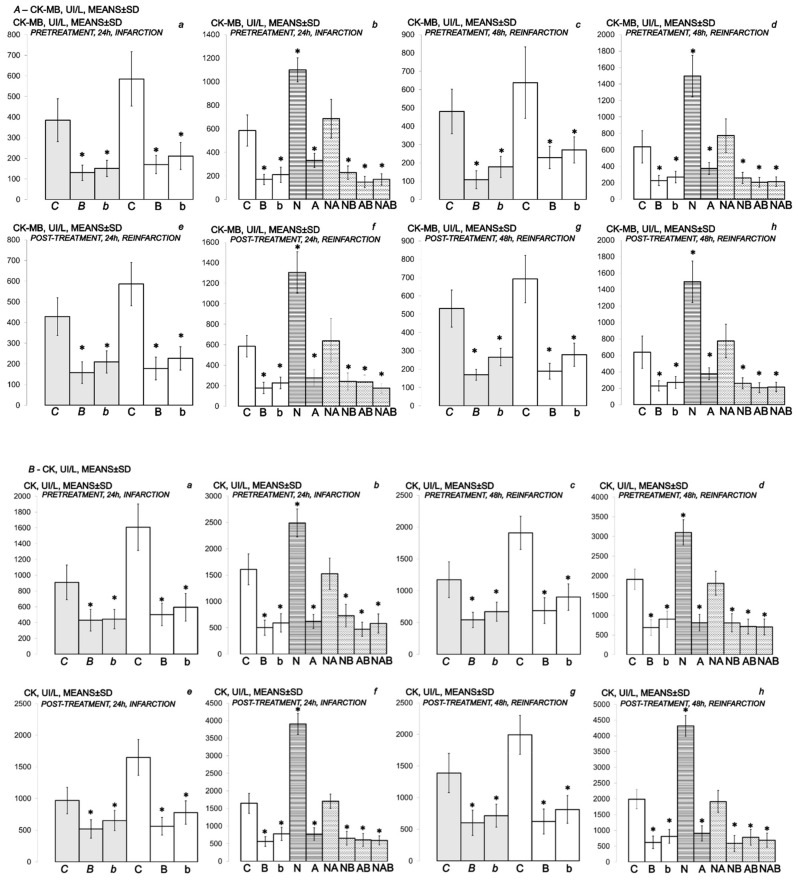
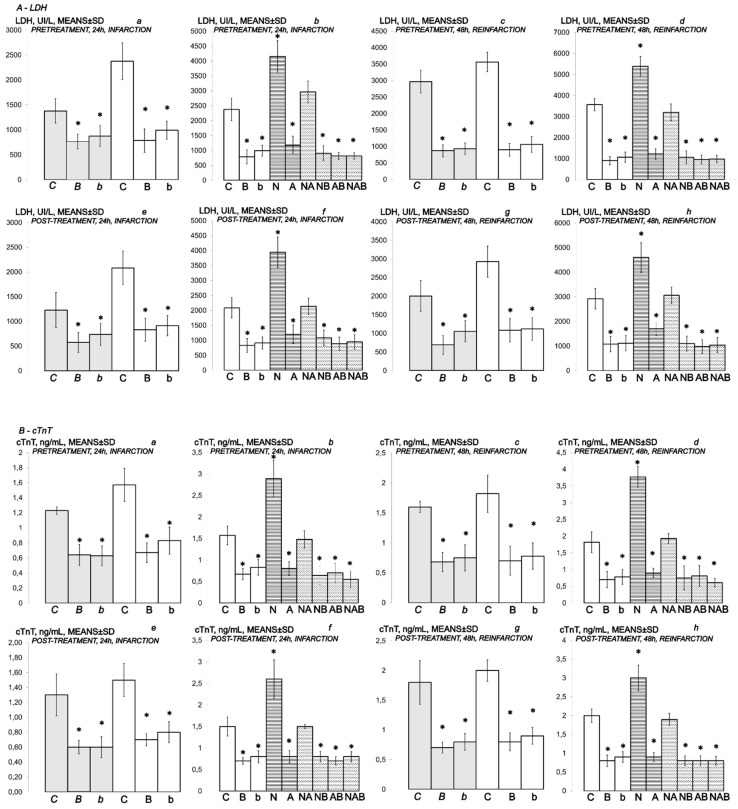
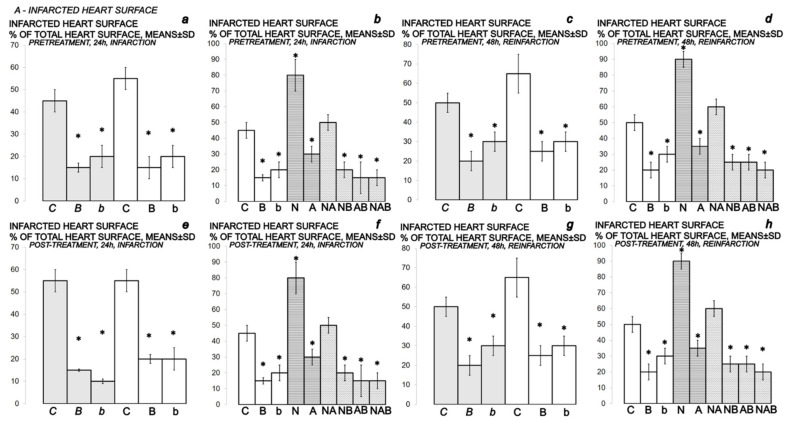
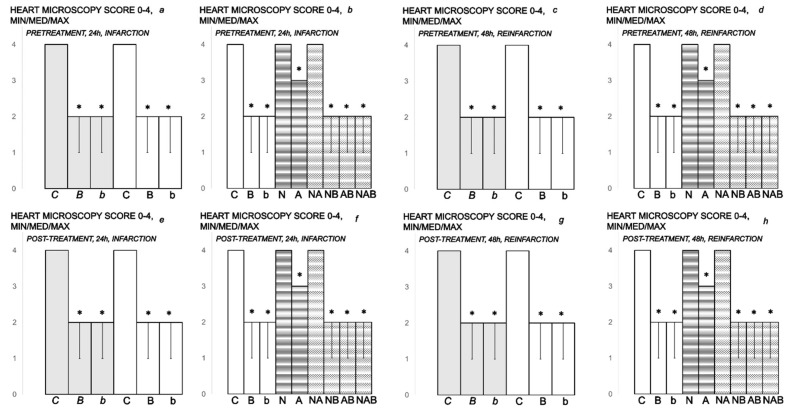
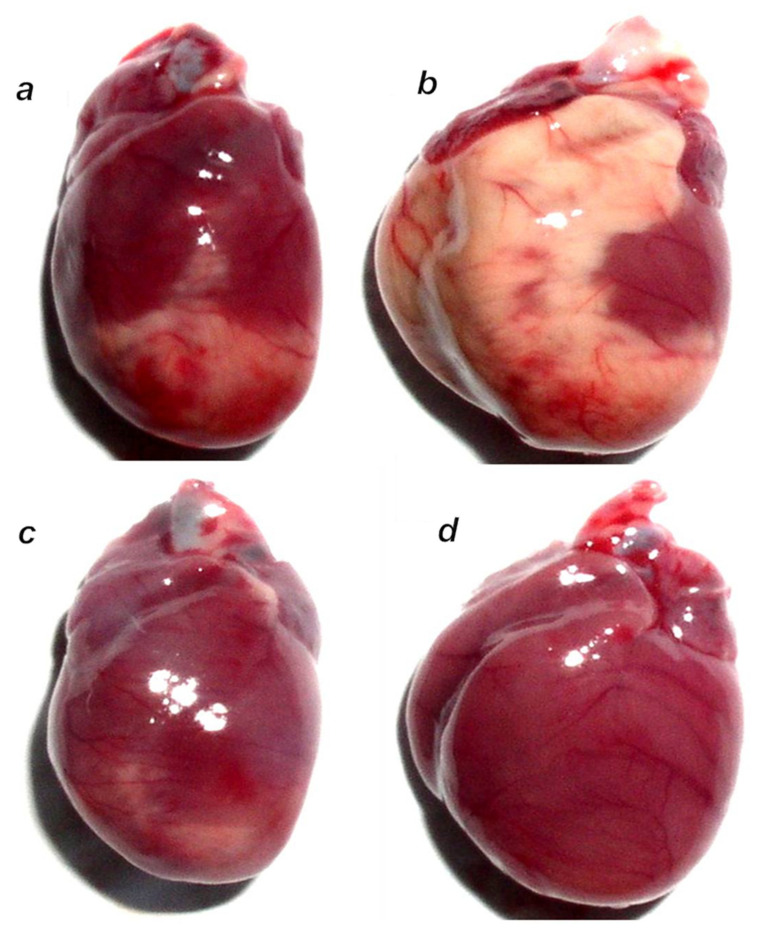
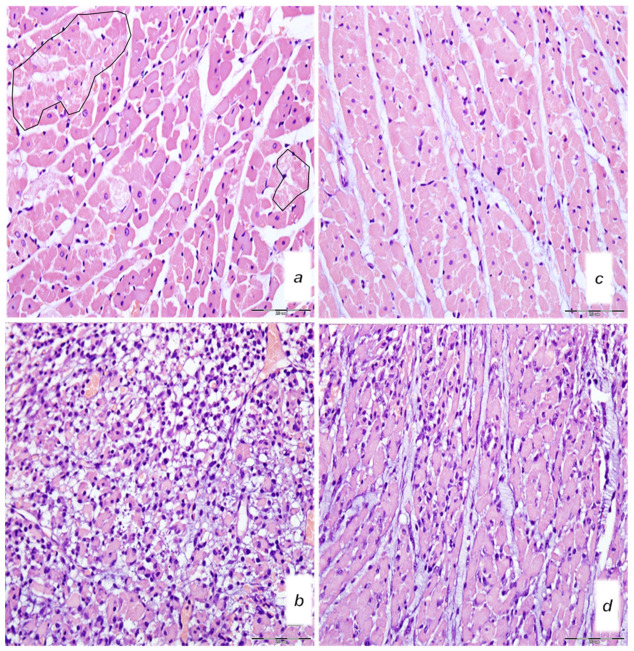
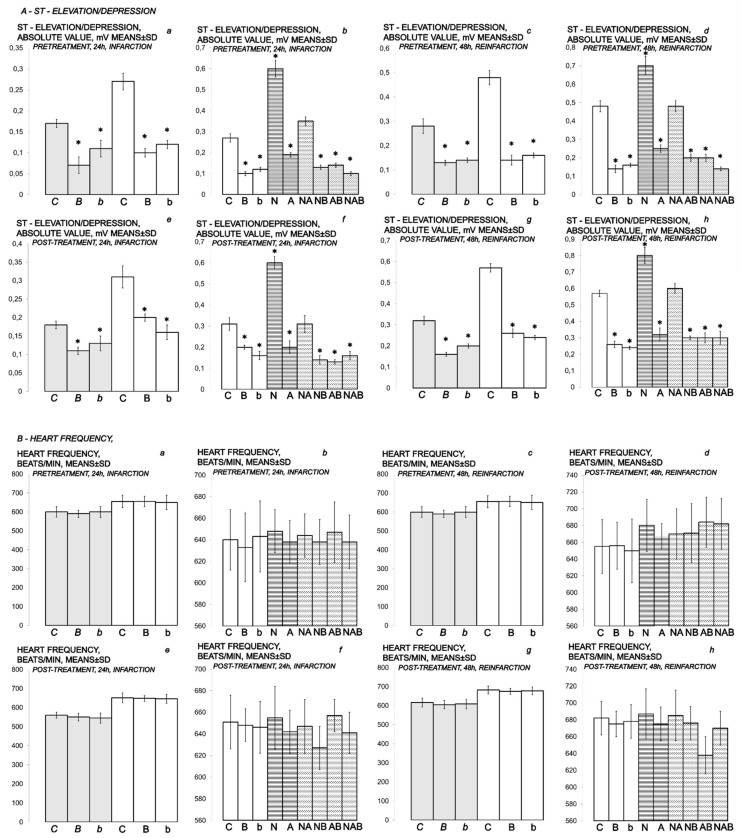
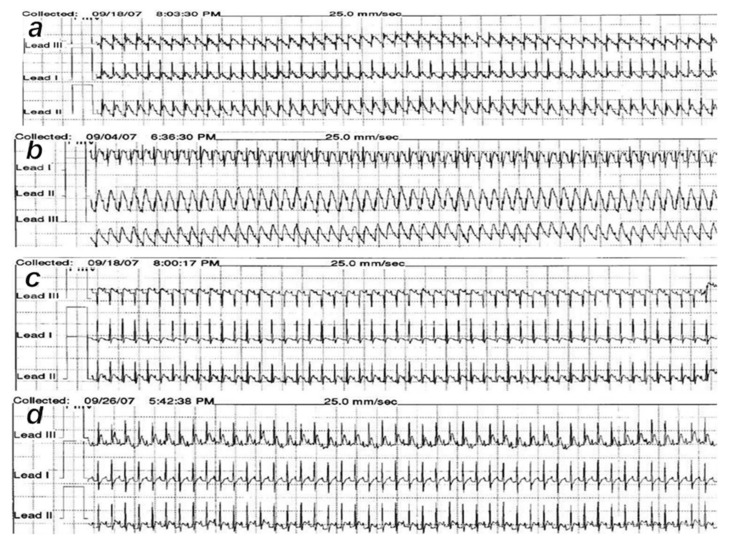
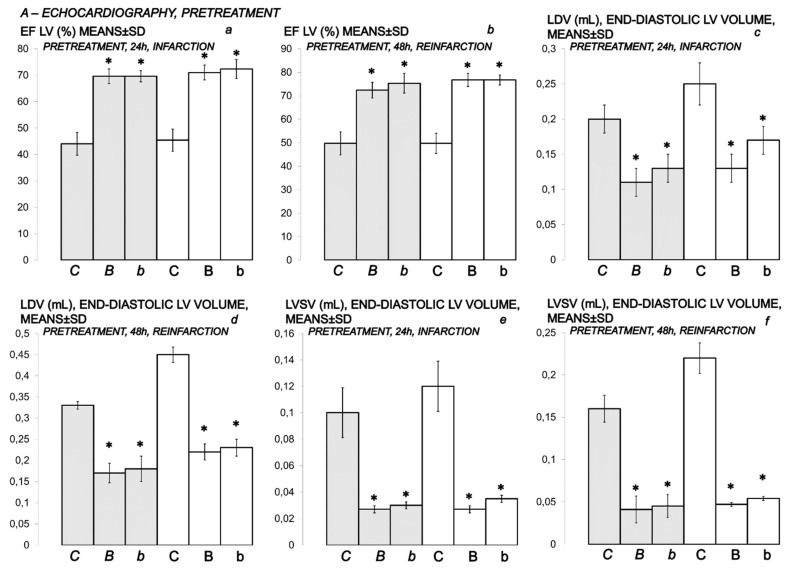
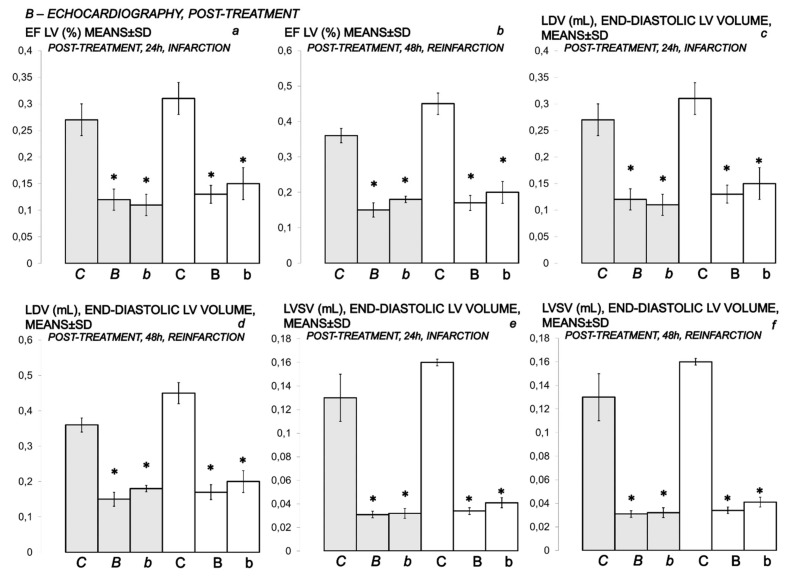
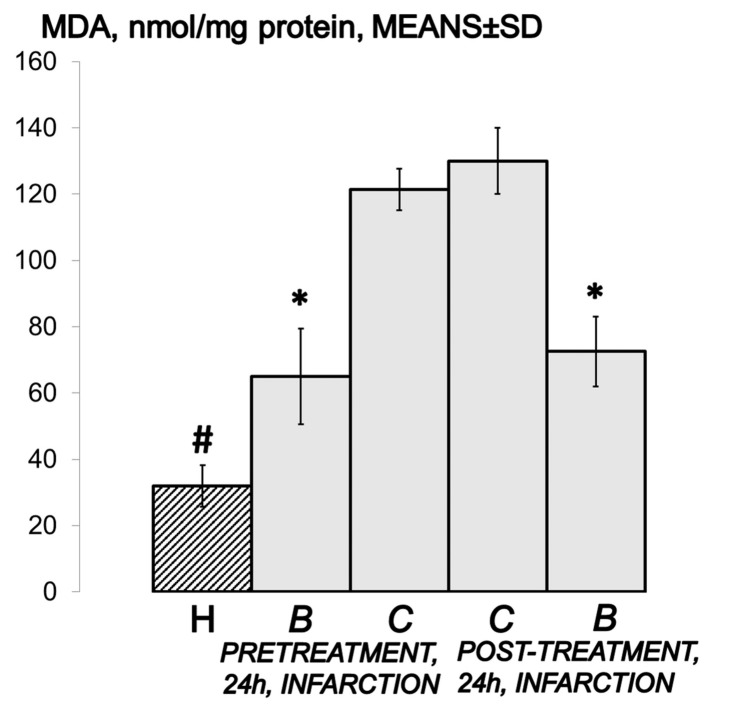
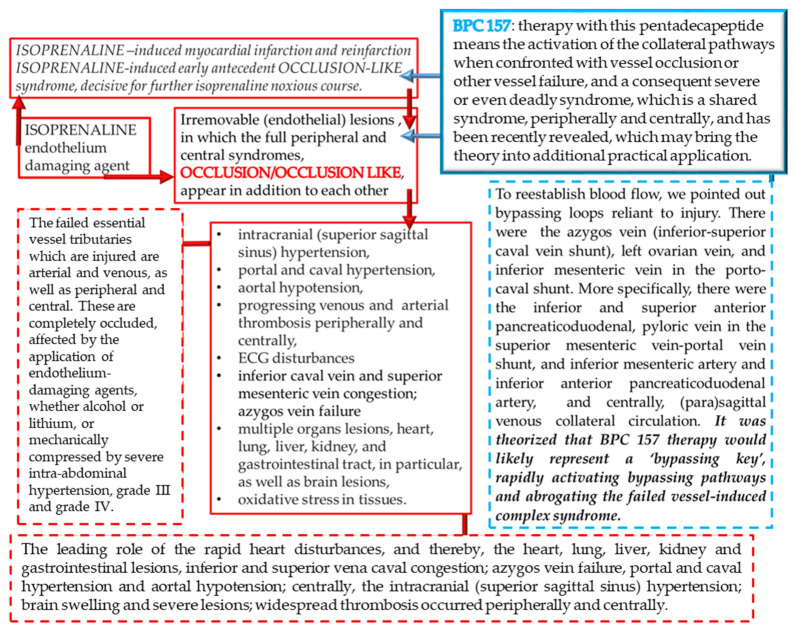
We revealed that the stable gastric pentadecapeptide BPC 157, a useful peptide therapy against isoprenaline myocardial infarction, as well as against isoprenaline myocardial reinfarction, may follow the counteraction of the recently described occlusion-like syndrome, induced peripherally and centrally, which was described for the first time in isoprenaline-treated rats. BPC 157 (10 ng/kg, 10 µg/kg i.p.), L-NAME (5 mg/kg i.p.), and L-arginine (200 mg/kg i.p.) were given alone or together at (i) 30 min before or, alternatively, (ii) at 5 min after isoprenaline (75 or 150 mg/kg s.c.). At 30 min after isoprenaline 75 mg/kg s.c., we noted an early multiorgan failure (brain, heart, lung, liver, kidney and gastrointestinal lesions), thrombosis, intracranial (superior sagittal sinus) hypertension, portal and caval hypertension, and aortal hypotension, in its full presentation (or attenuated by BPC 157 therapy (given at 5 min after isoprenaline) via activation of the azygos vein). Further, we studied isoprenaline (75 or 150 mg/kg s.c.) myocardial infarction (1 challenge) and reinfarction (isoprenaline at 0 h and 24 h, 2 challenges) in rats (assessed at the end of the subsequent 24 h period). BPC 157 reduced levels of all necrosis markers, CK, CK-MB, LDH, and cTnT, and attenuated gross (no visible infarcted area) and histological damage, ECG (no ST-T ischemic changes), and echocardiography (preservation of systolic left ventricular function) damage induced by isoprenaline. Its effect was associated with a significant decrease in oxidative stress parameters and likely maintained NO system function, providing that BPC 157 interacted with eNOS and COX2 gene expression in a particular way and counteracted the noxious effect of the NOS-blocker, L-NAME.
Keywords: L-NAME; L-arginine; isoprenaline; myocardial infarction; occlusion-like syndrome; oxidative stress; pentadecapeptide BPC 157; rats.
Conflict of interest statement
The authors declare that there are no conflict of interest.
Figures
References
-
- Sikiric P., Hahm K.-B., Blagaic A.B., Tvrdeic A., Pavlov K.H., Petrovic A., Kokot A., Gojkovic S., Krezic I., Drmic D., et al. Stable Gastric Pentadecapeptide BPC 157, Robert’s Stomach Cytoprotection/Adaptive Cytoprotection/Organoprotection, and Selye’s Stress Coping Response: Progress, Achievements, and the Future. Gut Liver. 2020;14:153–167. doi: 10.5009/gnl18490. - DOI - PMC - PubMed
-
- Sikiric P., Rucman R., Turkovic B., Sever M., Klicek R., Radic B., Drmic D., Stupnisek M., Misic M., Vuletic L.B., et al. Novel Cytoprotective Mediator, Stable Gastric Pentadecapeptide BPC Vascular Recruitment and Gastrointestinal Tract Healing. Curr. Pharm. Des. 2018;24:1990–2001. doi: 10.2174/1381612824666180608101119. - DOI - PubMed
-
- Lovric-Bencic M., Sikiric P., Hanzevacki J.S., Seiwerth S., Rogic D., Kusec V., Aralica G., Konjevoda P., Batelja L., Blagaic A.B. Doxorubicine-congestive heart failure-increased big endothelin-1 plasma concentration: Reversal by amlodipine, losartan, and gastric pentadecapeptide BPC157 in rat and mouse. J. Pharmacol. Sci. 2004;95:19–26. doi: 10.1254/jphs.95.19. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
