

The Diagnostic Deceiver: Radiological Pictorial Review of Tuberculosis
- PMID: 35204395
- PMCID: PMC8870832
- DOI: 10.3390/diagnostics12020306
The Diagnostic Deceiver: Radiological Pictorial Review of Tuberculosis
Abstract
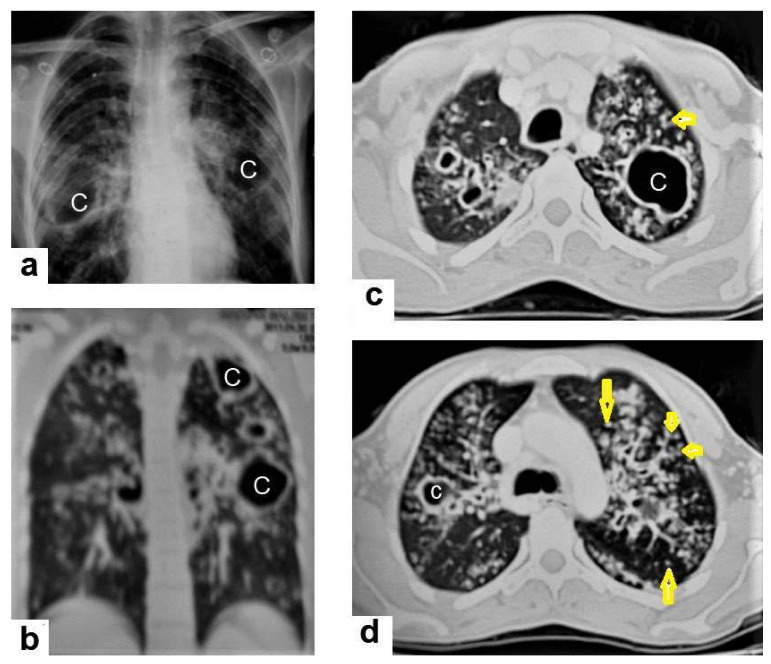
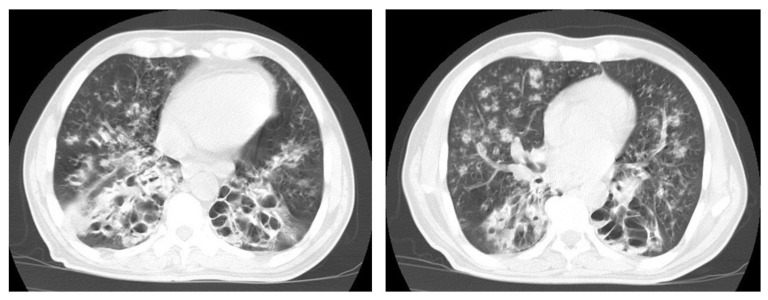
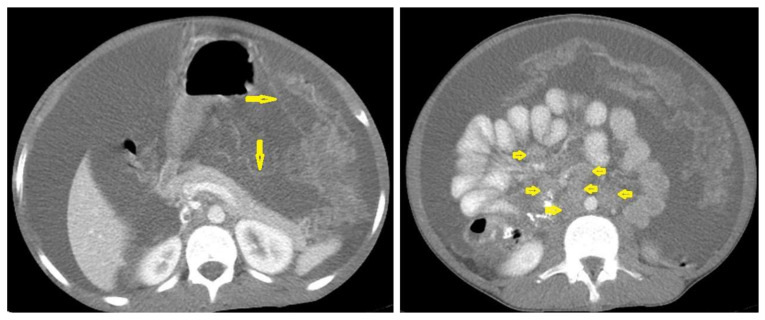
Tuberculosis (TB) is a bacterial infection with Mycobacterium tuberculosis; it is a public health problem worldwide and one of the leading causes of mortality. Since December 2019, the COVID-19 pandemic has created unprecedented health challenges and disrupted the TB health services, especially in high-burden countries with ever-increasing prevalence. Extrapulmonary and even pulmonary TB are an important cause of nonspecific clinical and radiological manifestations and can masquerade as any benign or malignant medical case, thus causing disastrous conditions and diagnostic dilemmas. Clinical manifestations and routine laboratory tests have limitations in directing physicians to diagnose TB. Medical-imaging examinations play an essential role in detecting tissue abnormalities and early suspecting diagnosis of TB in different organs. Radiologists and physicians should be familiar with and aware of the radiological manifestations of TB to contribute to the early suspicion and diagnosis of TB. The purpose of this article is to illustrate the common radiologic patterns of pulmonary and extrapulmonary TB. This article will be beneficial for radiologists, medical students, chest physicians, and infectious-disease doctors who are interested in the diagnosis of TB.
Keywords: cavitary lesions; miliary tuberculosis; tree-in-bud pattern; tuberculomas; tuberculous lymphadenitis; tuberculous pericarditis; tuberculous spondylitis.
Conflict of interest statement
The authors declare no conflict of interest.
Figures





















References
Publication types
LinkOut - more resources
Full Text Sources
