

MicroRNAs Related to TACE Treatment Response: A Review of the Literature from a Radiological Point of View
- PMID: 35204465
- PMCID: PMC8871153
- DOI: 10.3390/diagnostics12020374
MicroRNAs Related to TACE Treatment Response: A Review of the Literature from a Radiological Point of View
Abstract
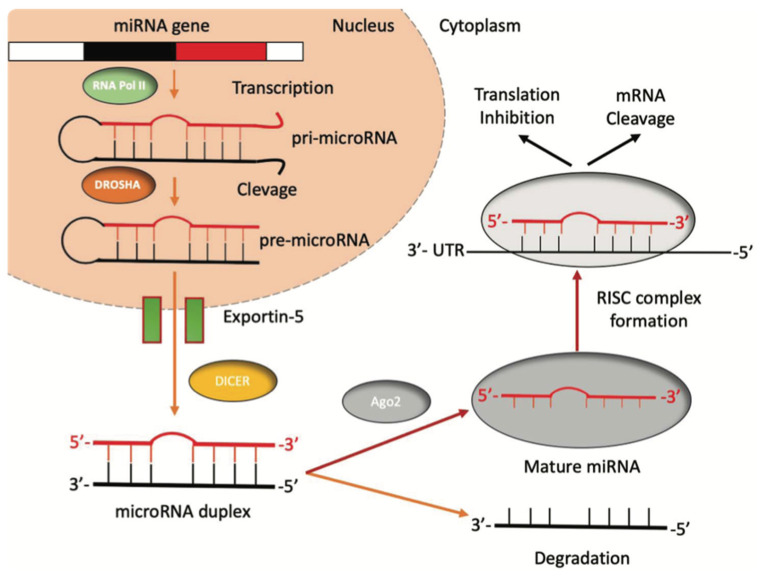
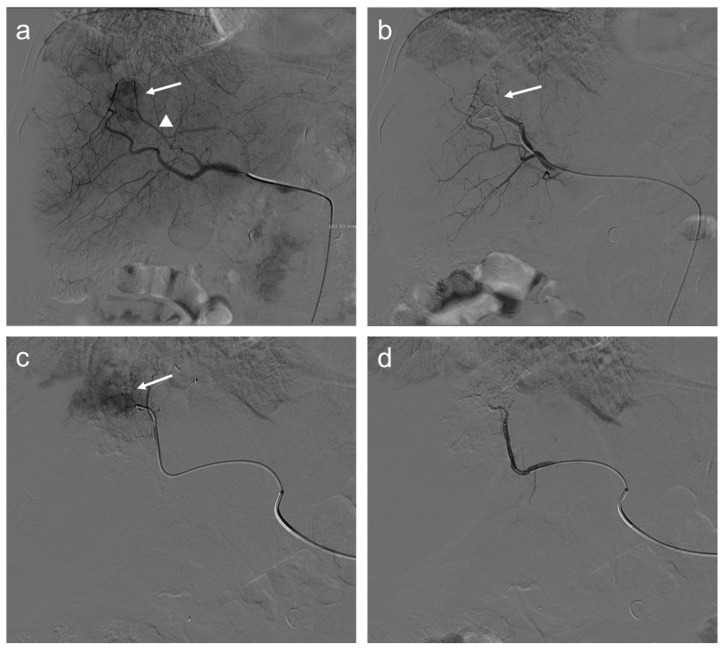
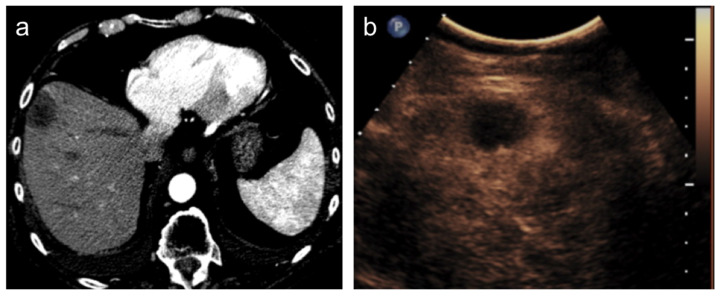
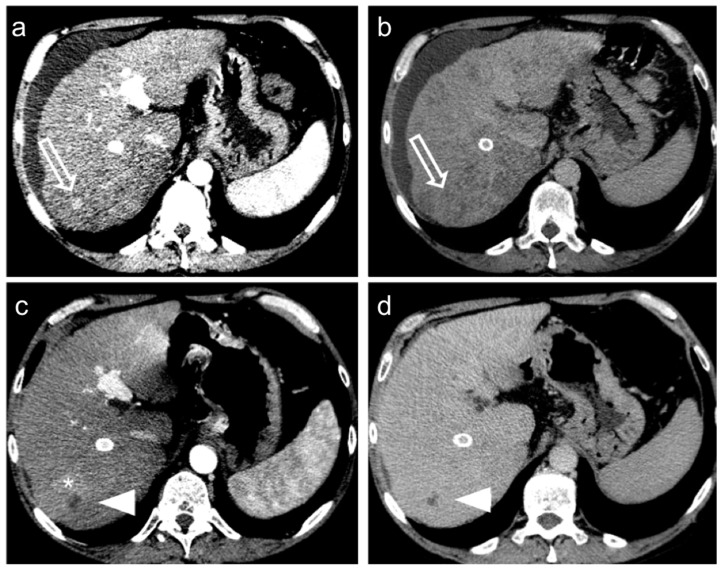
Hepatocellular Carcinoma (HCC) is the sixth most common cancer in the world. Patients with intermediate stage (Barcelona Clinic Liver Cancer, B stage) hepatocellular carcinoma (HCC) have been able to benefit from TACE (transarterial chemoembolization) as a treatment option. MicroRNAs (miRNAs), i.e., a subclass of non-coding RNAs (ncRNAs), participate in post-transcriptional gene regulation processes and miRNA dysfunction has been associated with apoptosis resistance, cellular proliferation, tumor genesis, and progression. Only a few studies have investigated the role of miRNAs as biomarkers predicting TACE treatment response in HCC. Here, we review the studies' characteristics from a radiological point of view, also correlating data with radiological images chosen from the cases of our institution.
Keywords: biomarkers; hepatocellular carcinoma (HCC); liver; liver cirrhosis; liver tumor; microRNA (miRNA); prognostic biomarkers; transarterial chemoembolization (TACE); treatment response criteria.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Campigotto M., Giuffrè M., Colombo A., Visintin A., Aversano A., Budel M., Masutti F., Abazia C., Crocé L.S. Comparison between hepatocellular carcinoma prognostic scores: A 10-year single-center experience and brief review of the current literature. World J. Hepatol. 2020;12:1239–1257. doi: 10.4254/wjh.v12.i12.1239. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
