

The Immune Landscape of Human Pancreatic Ductal Carcinoma: Key Players, Clinical Implications, and Challenges
- PMID: 35205742
- PMCID: PMC8870260
- DOI: 10.3390/cancers14040995
The Immune Landscape of Human Pancreatic Ductal Carcinoma: Key Players, Clinical Implications, and Challenges
Abstract
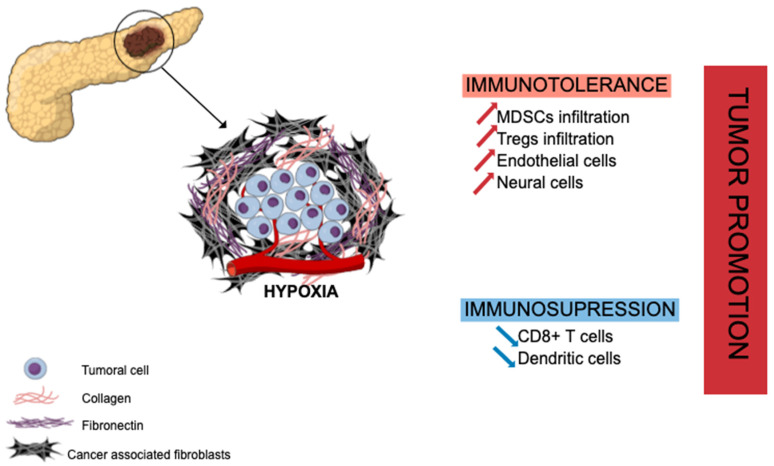
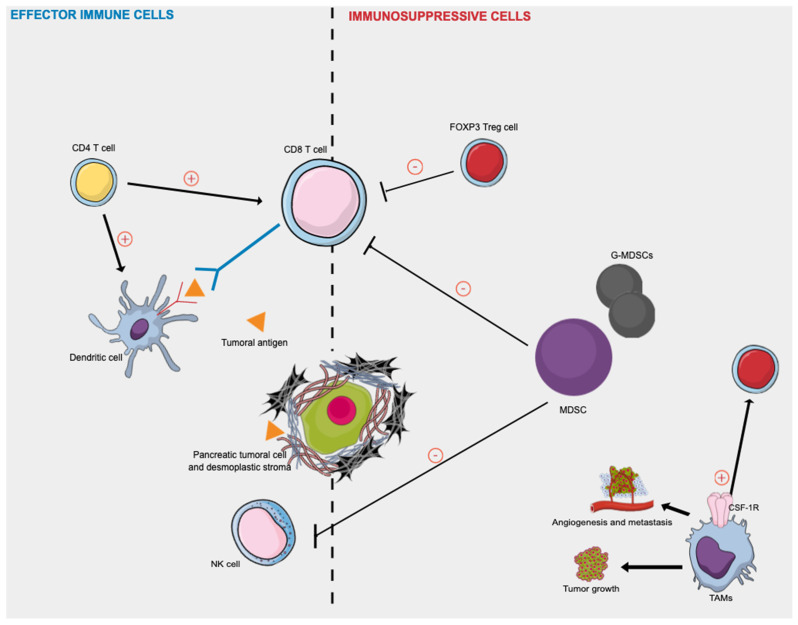
Pancreatic ductal adenocarcinoma (PDAC) is one of the most aggressive and deadliest cancer worldwide with an overall survival rate, all stages combined, of still <10% at 5 years. The poor prognosis is attributed to challenges in early detection, a low opportunity for radical resection, limited response to chemotherapy, radiotherapy, and resistance to immune therapy. Moreover, pancreatic tumoral cells are surrounded by an abundant desmoplastic stroma, which is responsible for creating a mechanical barrier, preventing appropriate vascularization and leading to poor immune cell infiltration. Accumulated evidence suggests that PDAC is impaired with multiple "immune defects", including a lack of high-quality effector cells (CD4, CD8 T cells, dendritic cells), barriers to effector cell infiltration due to that desmoplastic reaction, and a dominance of immune cells such as regulatory T cells, myeloid-derived suppressor cells, and M2 macrophages, resulting in an immunosuppressive tumor microenvironment (TME). Although recent studies have brought new insights into PDAC immune TME, its understanding remains not fully elucidated. Further studies are required for a better understanding of human PDAC immune TME, which might help to develop potent new therapeutic strategies by correcting these immune defects with the hope to unlock the resistance to (immune) therapy. In this review, we describe the main effector immune cells and immunosuppressive actors involved in human PDAC TME, as well as their implications as potential biomarkers and therapeutic targets.
Keywords: desmoplastic stroma; immune cells; pancreatic ductal adenocarcinoma; tumoral microenvironment.
Conflict of interest statement
The authors have no conflict of interest to declare.
Figures
References
-
- Arnold M., Rutherford M.J., Bardot A., Ferlay J., Andersson T.M.-L., Myklebust T.Å., Tervonen H., Thursfield V., Ransom D., Shack L., et al. Progress in Cancer Survival, Mortality, and Incidence in Seven High-Income Countries 1995–2014 (ICBP SURVMARK-2): A Population-Based Study. Lancet Oncol. 2019;20:1493–1505. doi: 10.1016/S1470-2045(19)30456-5. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
