

Regional Impact of COVID-19-Associated Pulmonary Aspergillosis (CAPA) during the First Wave
- PMID: 35205851
- PMCID: PMC8875881
- DOI: 10.3390/jof8020096
Regional Impact of COVID-19-Associated Pulmonary Aspergillosis (CAPA) during the First Wave
Abstract
Background: Critically ill COVID-19 patients have proven to be at risk for developing invasive fungal infections. However, the incidence and impact of possible/probable COVID-19-associated pulmonary aspergillosis (CAPA) in severe COVID-19 patients varies between cohorts. We aimed to assess the incidence, risk factors, and clinical outcome of invasive pulmonary aspergillosis in a regional cohort of COVID-19 intensive care patients.
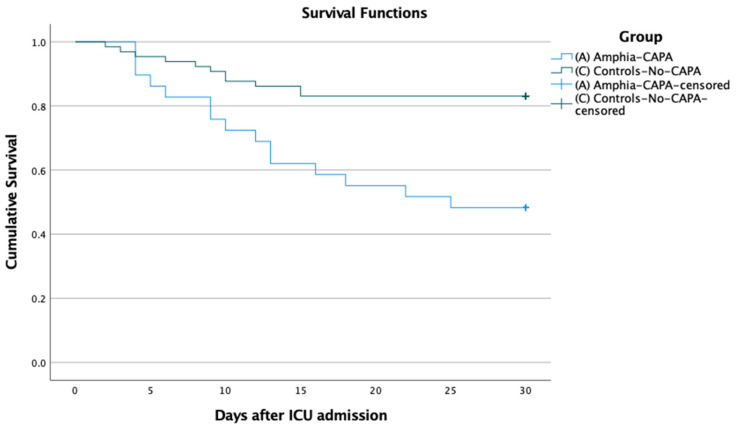
Methods: We performed a regional, multicentre, retrospective cohort study in the intensive care units (ICUs) in North Brabant, The Netherlands. We included adult patients with rt-PCR-confirmed SARS-CoV-2 infection (COVID-19), requiring mechanical ventilation for acute respiratory distress syndrome. Demographics, clinical course, biomarker value, and treatment outcomes were compared between the groups with possible/probable CAPA from the main study centre and the regional centres, and without signs of CAPA from the main study centre as controls. The primary aim was to assess the regional impact of possible/probable CAPA in COVID-19 ICU patients, measured as all-cause mortality at 30 days after ICU admission. Secondary outcomes were risk factors for developing CAPA, based on underlying host factors and to identify the value of the mycological arguments for the diagnosing of CAPA.
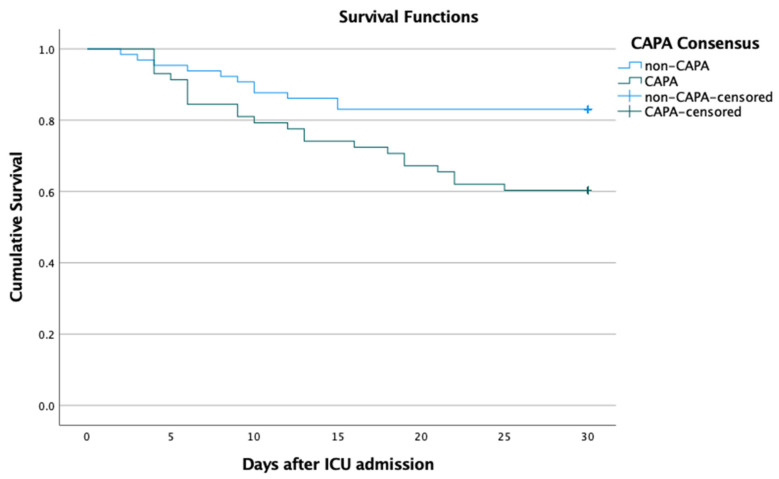
Results: Between 1 March and 30 April 2020, we included 123 patients with severe COVID-19: 29 patients (30.9%) in the main ICU with possible/probable CAPA, and 65 (69.1%) with no signs of CAPA; 29 patients in the regional ICUs with signs of CAPA. Patients' characteristics and risk factors did not differ for CAPA and non-CAPA patients. Patients with COPD and/or chronic steroid medication developed CAPA more frequently, although this was not statistically significant. CAPA patients were admitted to the ICU earlier, had lower PF-ratios, and more often required renal replacement therapy. All-cause 30-day mortality was significantly higher in mechanically ventilated COVID-19 patients with possible/probable CAPA 39.7% (23/58) compared to patients without evidence for CAPA 16.9% (11/65) (OR 3.2 [95% CI 1.4-7.4] p = 0.005).
Conclusion: The high incidence of possible and probable CAPA in critically ill COVID-19 patients is alarming. The increase in 30-day mortality in CAPA highlights the need for active surveillance and management strategies in critically ill COVID-19 patients.
Keywords: CAPA; COVID-19; corticosteroids; pulmonary aspergillosis; voriconazole.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Zhou F., Yu T., Du R., Fan G., Liu Y., Liu Z., Xiang J., Wang Y., Song B., Gu X., et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet. 2020;395:1054–1062. doi: 10.1016/S0140-6736(20)30566-3. - DOI - PMC - PubMed
-
- Van der Moeren N., Talman S., van den Bijllaardt W., Kant M., Heukels P., Bentvelsen R.G., Loth D.W. The first 29 COVID-19-patients in a clinic: Early experiences from a Dutch hospital. Ned. Tijdschr. Geneeskd. 2020;164:D4981. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
