

A Novel Doppler TRPG/AcT Index Improves Echocardiographic Diagnosis of Pulmonary Hypertension after Pulmonary Embolism
- PMID: 35207345
- PMCID: PMC8879629
- DOI: 10.3390/jcm11041072
A Novel Doppler TRPG/AcT Index Improves Echocardiographic Diagnosis of Pulmonary Hypertension after Pulmonary Embolism
Abstract
Background: We hypothesized that a Doppler index, the ratio of tricuspid regurgitation peak gradient (TRPG) to pulmonary ejection acceleration time (AcT), improves the assessment of the echocardiographic probability of pulmonary hypertension in the identification of CTEPH and chronic thromboembolic pulmonary disease (CTED) in symptomatic patients after PE. Doppler echocardiography is recommended as the initial imaging tool for the diagnosis of chronic thromboembolic pulmonary hypertension (CTEPH) after acute pulmonary embolism (PE).
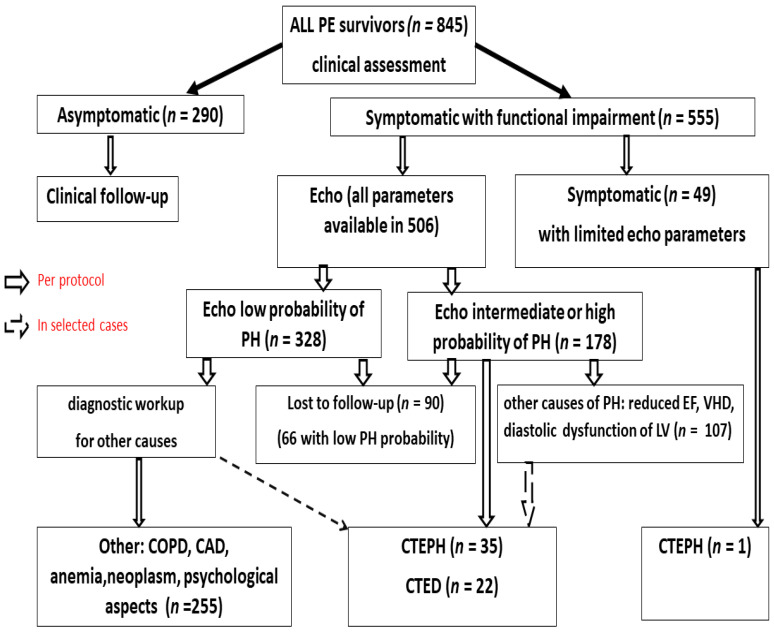
Methods: We analyzed the data from 845 consecutive PE (468 women; 61 ± 18 years) survivors who completed at least 6 months of anticoagulation therapy. Here, 555 patients (325 women; 66 ± 16 years) reporting functional impairment (FI) underwent transthoracic echocardiography. We included 506 patients (297 women; age 63.4 ± 16.6 years) in whom both AcT and TRPG were available into the current study. The presence of a minimum of intermediate echocardiographic probability of PH necessitated the diagnosis of CTEPH.
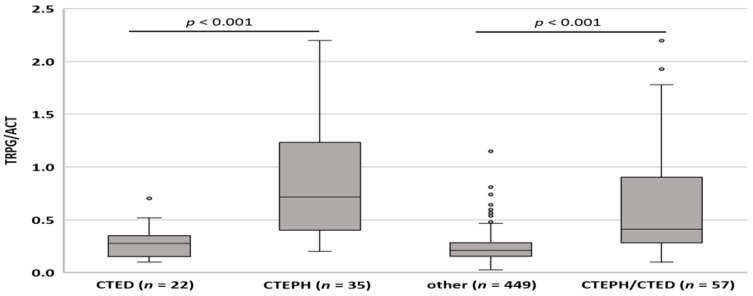
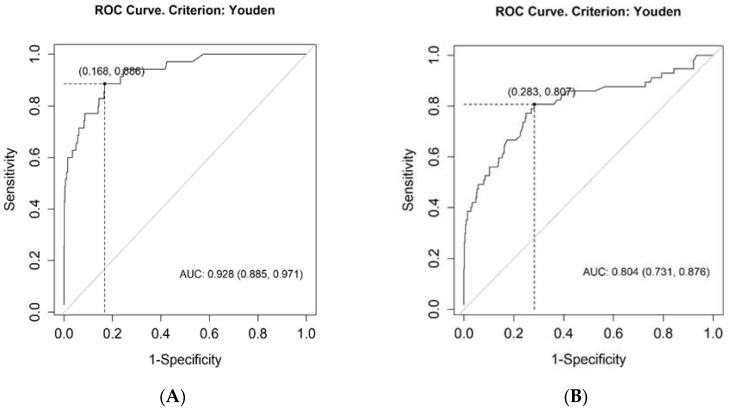
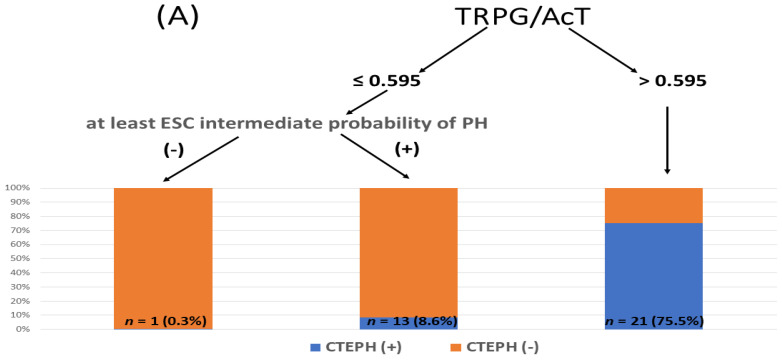
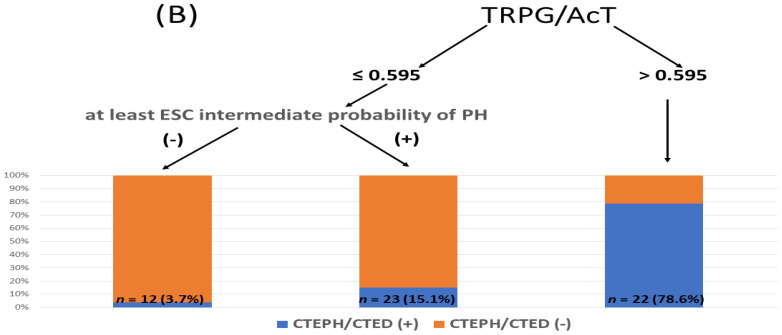
Results: Echocardiography revealed a high echocardiographic probability of PH in 69 (13.6%) and intermediate echocardiographic probability in 109 (21.5%) patients. CTEPH was diagnosed in 35 (6.9%) patients and CTED in 22 (4.3%) patients. TRPG/AcT was significantly higher in the combined CTEPH + CTED group than in those with other causes of FI (0.412 (0.100-2.197) vs. 0.208 (0.026-0.115), p < 0.001), and the area under the receiver operating characteristic curve of the TRPG/AcT for CTEPH + CTED was 0.804 (95% confidence interval (CI): 0.731-0.876). Importantly, multiple logistic regression showed that TRPG/AcT is a significant predictor of CTEPH + CTED after considering echocardiographic probability (odds ratio = 1.51, 95% CI: 1.25-1.91, p < 0.001). Conditional inference trees analysis revealed that TRPG/AcT > 0.595 identified patients with CTEPH or CTED with a positive predictive value of 78.6% and negative predictive value of 92.7%.
Conclusions: A Doppler index TRPG/AcT improves the assessment of symptomatic PE survivors. TRPG/AcT > 0.6 indicates a high probability of CTEPH or CTED, whereas TRPG/AcT < 0.6 allows for the safe exclusion of CTEPH + CTED in patients with a low echocardiographic probability of PH.
Keywords: chronic thromboembolic pulmonary hypertension; echocardiographic probability of pulmonary hypertension; echocardiography; pulmonary embolism.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Klok F.A., Barco S. Follow-up after acute Pulmonary Embolism. Hamostaseologie. 2018;38:22–32. - PubMed
-
- Dzikowska-Diduch O., Kostrubiec M., Kurnicka K., Lichodziejewska B., Pacho S., Miroszewska A., Bródka K., Skowrońska M., Łabyk A., Roik M., et al. The post-pulmonary syndrome—Results of echocardiographic driven follow up after acute pulmonary embolism. Thromb. Res. 2020;186:30–35. doi: 10.1016/j.thromres.2019.12.008. - DOI - PubMed
-
- Kahn S.R., Comerota A.J., Cushman M., Evans N.S., Ginsberg J.S., Goldenberg N.A., Gupta D.K., Prandoni P., Vedantham S., Walsh M.E., et al. The postthrombotic syndrome: Evidence-based prevention, diagnosis, and treatment strategies: A scientific statement from the American Heart Association. Circulation. 2014;130:1636–1661. doi: 10.1161/CIR.0000000000000130. - DOI - PubMed
-
- Ende-Verhaar Y.M., Cannegieter S.C., Vonk Noordegraaf A., Delcroix M., Pruszczyk P., Mairuhu A.T., Huisman M.V., Klok F.A. Incidence of chronic thromboembolic pulmonary hypertension after acute pulmonary embolism: A contemporary view of the published literature. Eur. Respir. J. 2017;49:1601792. doi: 10.1183/13993003.01792-2016. - DOI - PubMed
LinkOut - more resources
Full Text Sources
