

Immunotherapeutic Approaches for the Treatment of HPV-Associated (Pre-)Cancer of the Cervix, Vulva and Penis
- PMID: 35207374
- PMCID: PMC8876514
- DOI: 10.3390/jcm11041101
Immunotherapeutic Approaches for the Treatment of HPV-Associated (Pre-)Cancer of the Cervix, Vulva and Penis
Abstract
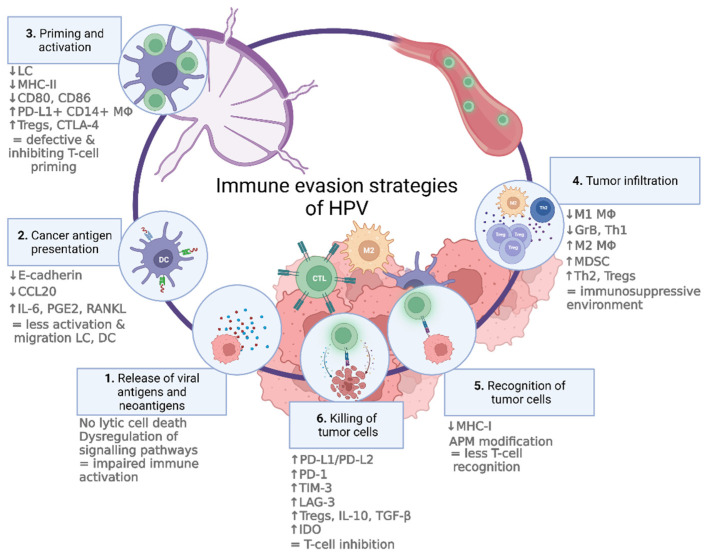
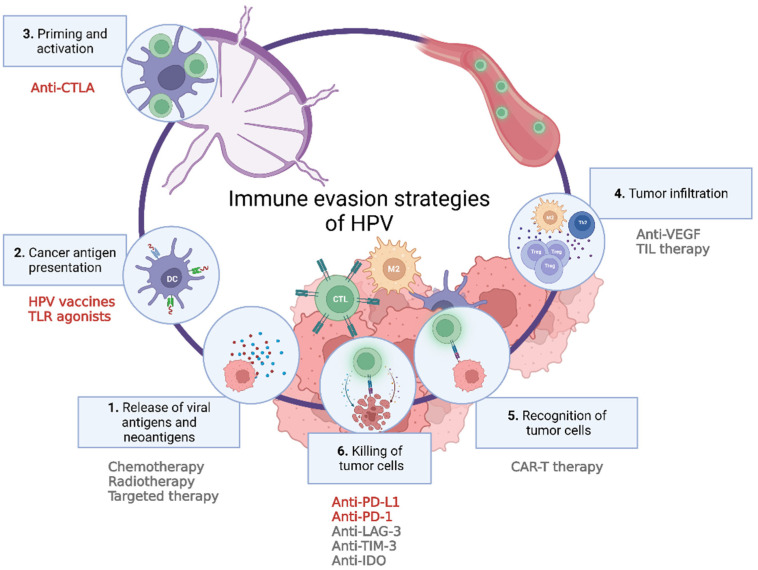
Human papillomavirus (HPV) infection drives tumorigenesis in almost all cervical cancers and a fraction of vulvar and penile cancers. Due to increasing incidence and low vaccination rates, many will still have to face HPV-related morbidity and mortality in the upcoming years. Current treatment options (i.e., surgery and/or chemoradiation) for urogenital (pre-)malignancies can have profound psychosocial and psychosexual effects on patients. Moreover, in the setting of advanced disease, responses to current therapies remain poor and nondurable, highlighting the unmet need for novel therapies that prevent recurrent disease and improve clinical outcome. Immunotherapy can be a useful addition to the current therapeutic strategies in various settings of disease, offering relatively fewer adverse effects and potential improvement in survival. This review discusses immune evasion mechanisms accompanying HPV infection and HPV-related tumorigenesis and summarizes current immunotherapeutic approaches for the treatment of HPV-related (pre-)malignant lesions of the uterine cervix, vulva, and penis.
Keywords: cervical cancer; human papillomavirus; immunotherapy; penile cancer; urogenital; vulvar cancer.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
