

Lipoprotein(a), Immune Cells and Cardiovascular Outcomes in Patients with Premature Coronary Heart Disease
- PMID: 35207757
- PMCID: PMC8876319
- DOI: 10.3390/jpm12020269
Lipoprotein(a), Immune Cells and Cardiovascular Outcomes in Patients with Premature Coronary Heart Disease
Abstract
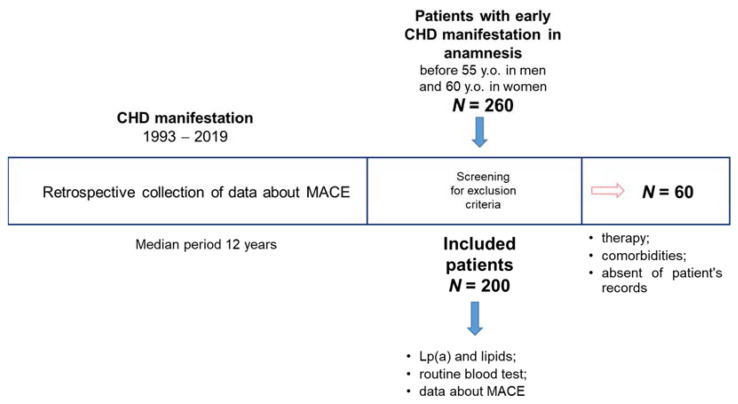
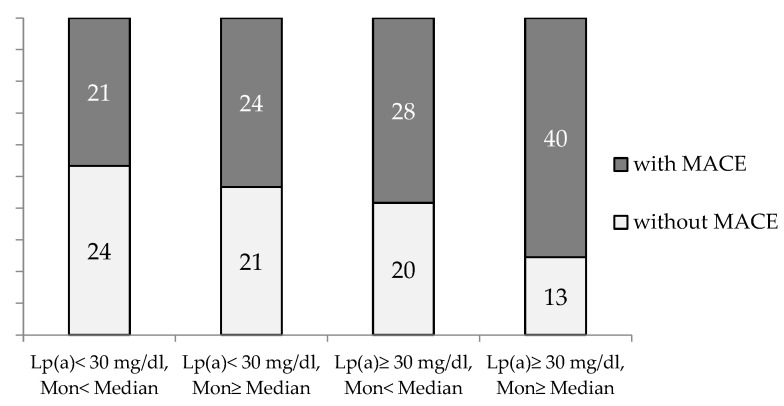
The detection of lipoprotein(a) [Lp(a)] in the artery wall at the stage of lipid-bands formation may indicate that it participates in the atherosclerosis local nonspecific inflammatory process. Innate immune cells are involved in atherogenesis, with monocytes playing a major role in the initiation of atherosclerosis, while neutrophils can contribute to plaque destabilization. This work studies the relationship between Lp(a), immune blood cells and major adverse cardiovascular events (MACE) in patients with the early manifestation of coronary heart disease (CHD). The study included 200 patients with chronic CHD, manifested up to the age of 55 in men and 60 in women. An increased Lp(a) concentration [hyperLp(a)] was shown to predict cardiovascular events in patients with premature CHD with long-term follow-up. According to the logistic regression analysis results, an increase in the monocyte count with OR = 4.58 (95% CI 1.04-20.06) or lymphocyte-to-monocyte ratio with OR = 0.82 (0.68-0.99), (p < 0.05 for both) was associated with MACE in patients with early CHD, regardless of gender, age, classical risk factors, atherogenic lipoproteins concentration and statin intake. The combination of an increased monocyte count and hyperLp(a) significantly increased the proportion of patients with early CHD with subsequent development of MACE (p = 0.02, ptrend = 0.003). The odds of cardiovascular events in patients with early CHD manifestation were highest in patients with an elevated lymphocyte-to-monocyte ratio and an elevated Lp(a) level. A higher neutrophil blood count and an elevated neutrophil-to-lymphocyte ratio determined the faster development of MACE in patients with a high Lp(a) concentration. The data obtained in this study suggest that the high atherothrombogenicity of Lp(a) is associated with the "inflammatory" component and the innate immune cells involvement in this process. Thus, the easily calculated immunological ratios of blood cells and Lp(a) concentrations can be considered simple predictors of future cardiovascular events.
Keywords: coronary heart disease; immune cells blood count; lipoprotein(a).
Conflict of interest statement
The authors declare no conflict of interest.
Figures






References
-
- WHO . The Top 10 Causes of Death. World Health Organization; Geneva, Switzerland: 2018.
-
- Maillet A., Desormais I., Rivière A.B., Aboyans V., Lacroix P., Mirault T., Messas E., Bataille V., Constans J., Boulon C. Peripheral Atheromatous Arterial Disease in the Young: Risk Factors, Clinical Features, and Prognosis from the COPART Cohort. Angiology. 2017;68:893–898. doi: 10.1177/0003319717699501. - DOI - PubMed
-
- Tibæk M., Dehlendorff C., Jørgensen H.S., Forchhammer H.B., Johnsen S.P., Kammersgaard L.P. Increasing Incidence of Hospitalization for Stroke and Transient Ischemic Attack in Young Adults: A Registry-Based Study. J. Am. Heart Assoc. 2016;5:e003158. doi: 10.1161/JAHA.115.003158. - DOI - PMC - PubMed
-
- Vikulova D.N., Grubisic M., Zhao Y., Lynch K., Humphries K.H., Pimstone S.N., Brunham L.R. Premature Atherosclerotic Cardiovascular Disease: Trends in Incidence, Risk Factors, and Sex-Related Differences, 2000 to 2016. J. Am. Heart Assoc. 2019;8:e012178. doi: 10.1161/JAHA.119.012178. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
