

A Potential Role for Bile Acid Signaling in Celiac Disease-Associated Fatty Liver
- PMID: 35208205
- PMCID: PMC8879761
- DOI: 10.3390/metabo12020130
A Potential Role for Bile Acid Signaling in Celiac Disease-Associated Fatty Liver
Abstract
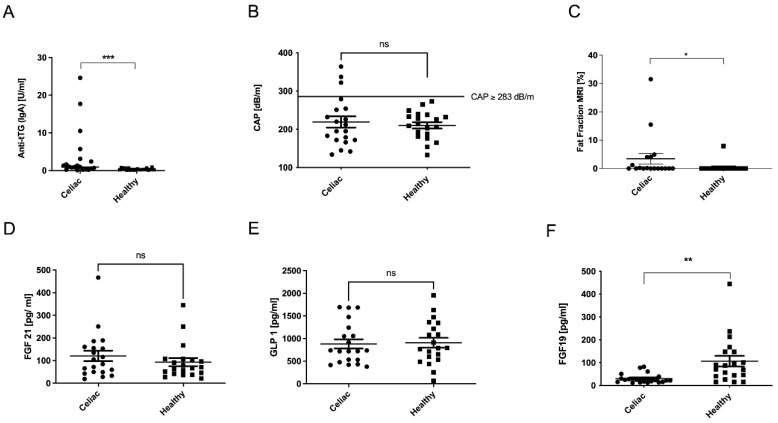
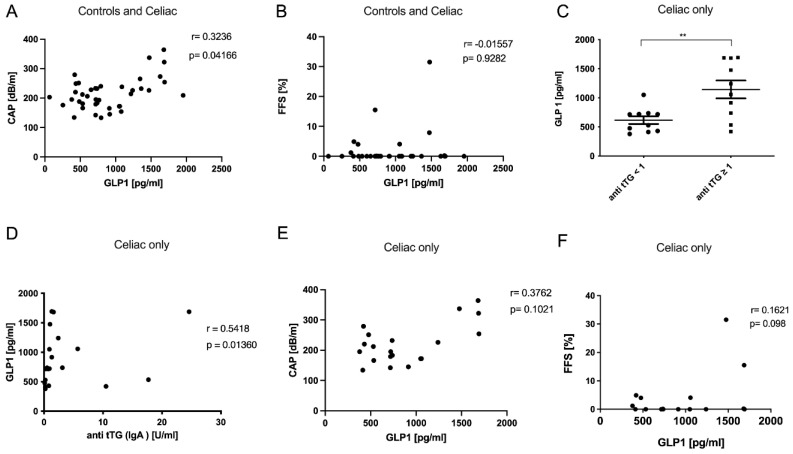
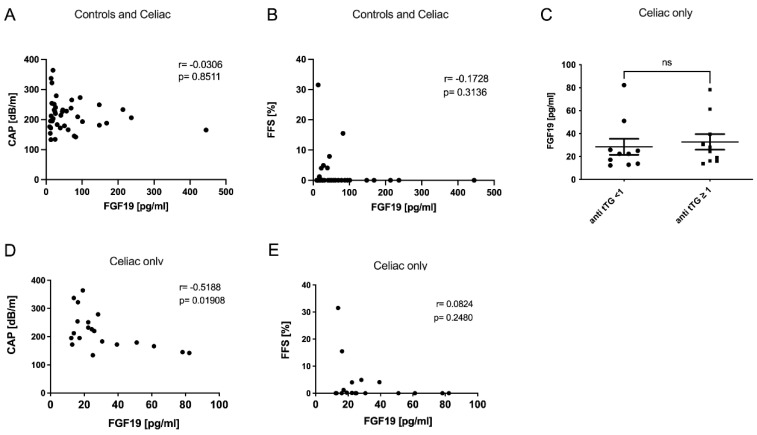
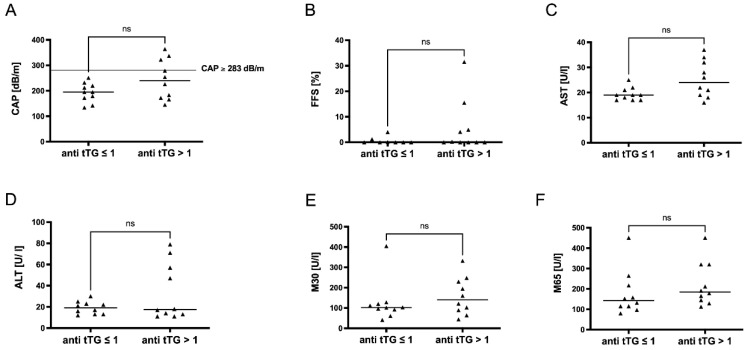
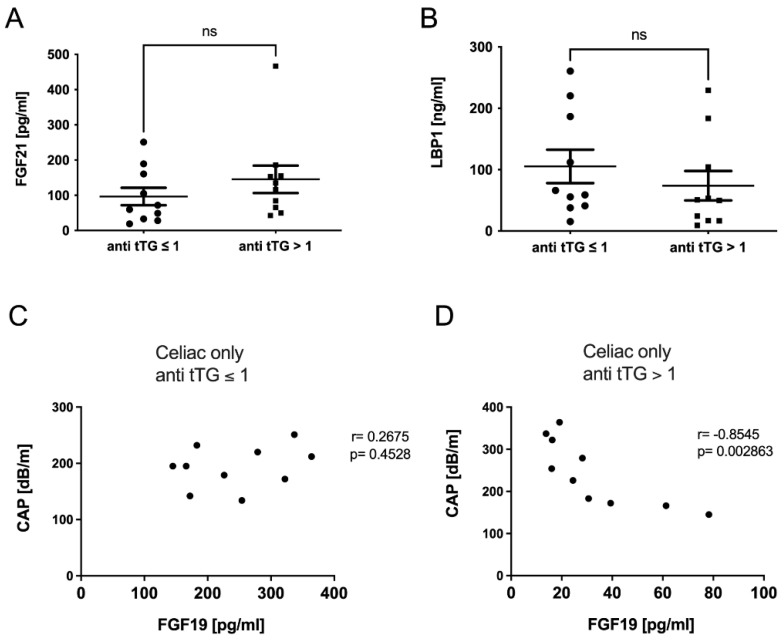
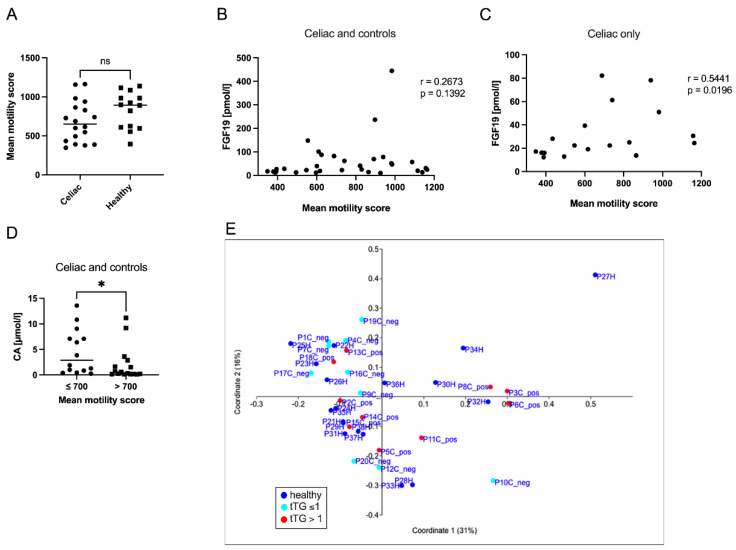
Celiac disease (CeD) is a chronic autoimmune disorder characterized by an intolerance to storage proteins of many grains. CeD is frequently associated with liver damage and steatosis. Bile acid (BA) signaling has been identified as an important mediator in gut-liver interaction and the pathogenesis of non-alcoholic fatty liver disease (NAFLD). Here, we aimed to analyze BA signaling and liver injury in CeD patients. Therefore, we analyzed data of 20 CeD patients on a gluten-free diet compared to 20 healthy controls (HC). We furthermore analyzed transaminase levels, markers of cell death, BA, and fatty acid metabolism. Hepatic steatosis was determined via transient elastography, by MRI and non-invasive scores. In CeD, we observed an increase of the apoptosis marker M30 and more hepatic steatosis as compared to HC. Fibroblast growth factor 19 (FGF19) was repressed in CeD, while low levels were associated with steatosis, especially in patients with high levels of anti-tissue transglutaminase antibodies (anti-tTG). When comparing anti-tTG-positive CeD patients to individuals without detectable anti-tTG levels, hepatic steatosis was accentuated. CeD patients with significant sonographic steatosis (defined by CAP ≥ 283 db/m) were exclusively anti-tTG-positive. In summary, our results suggest that even in CeD patients in clinical remission under gluten-free diet, alterations in gut-liver axis, especially BA signaling, might contribute to steatotic liver injury and should be further addressed in future studies and clinical practice.
Keywords: FGF19; bile acids; celiac disease; hepatic steatosis; non-alcoholic fatty liver disease (NAFLD).
Conflict of interest statement
All authors declare that they do not have a conflict of interests.
Figures
References
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
