

Diagnosis and Treatment of Primary Inflammatory Choriocapillaropathies (PICCPs): A Comprehensive Overview
- PMID: 35208488
- PMCID: PMC8879059
- DOI: 10.3390/medicina58020165
Diagnosis and Treatment of Primary Inflammatory Choriocapillaropathies (PICCPs): A Comprehensive Overview
Abstract
Purpose: Primary inflammatory choriocapillaropathies (PICCPs) belong to a group of intraocular inflammatory diseases with the common characteristic of inflammatory choriocapillaris hypo- or non-perfusion as the main clinicopathological mechanism. The purpose of our article is to describe clinical characteristics and multimodal imaging, that can help the diagnosis and treatment of PICCPs.
Methods: Narrative review with multimodal imaging analysis.
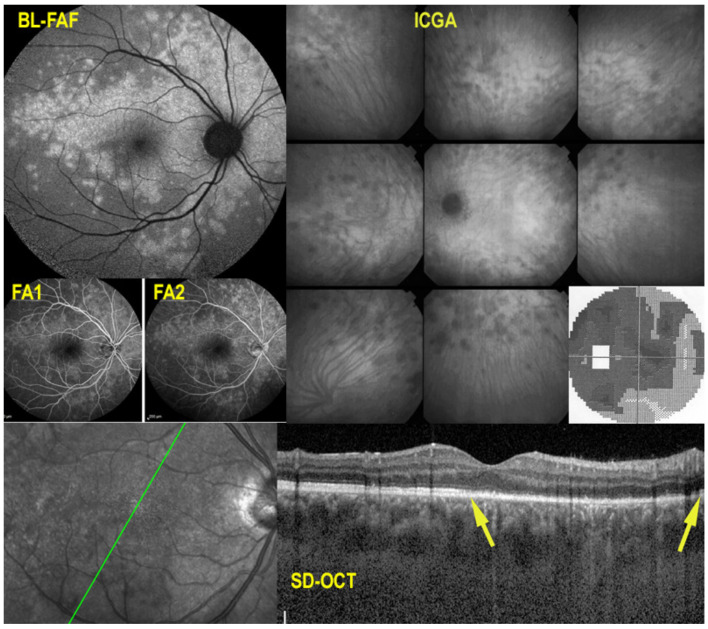
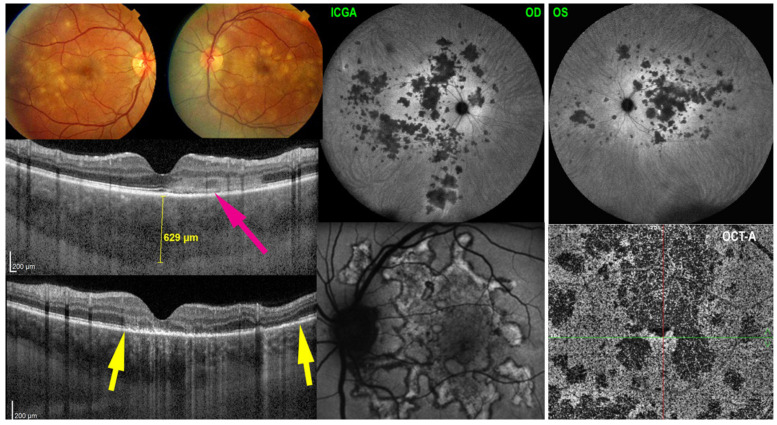
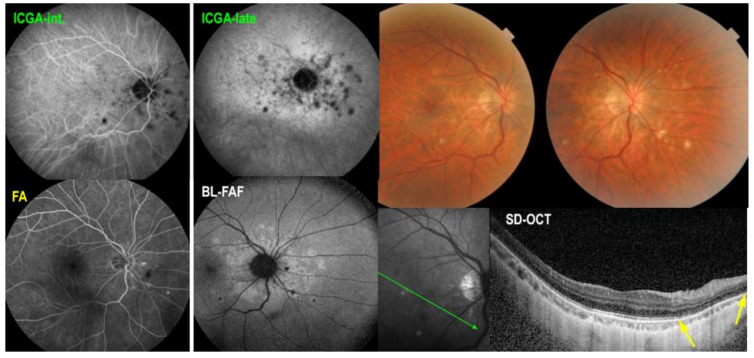
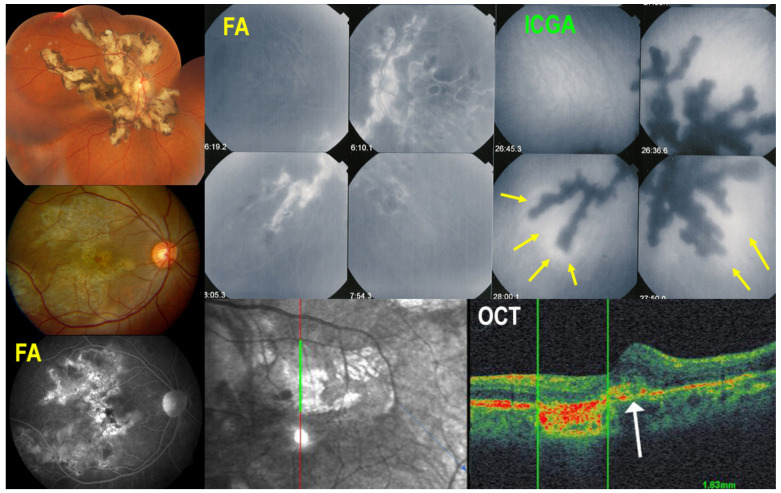
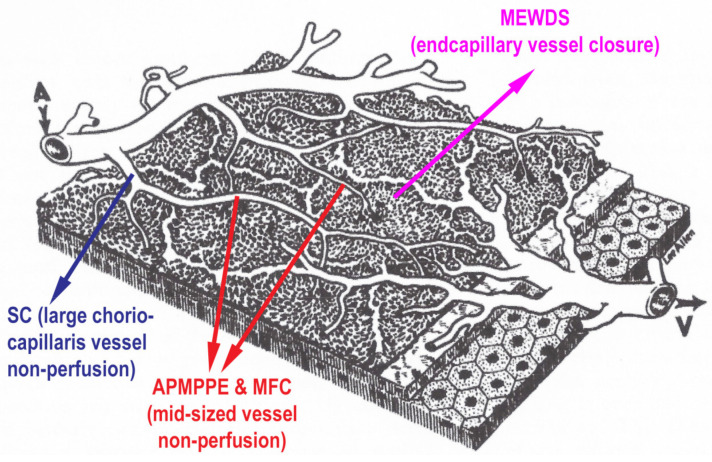
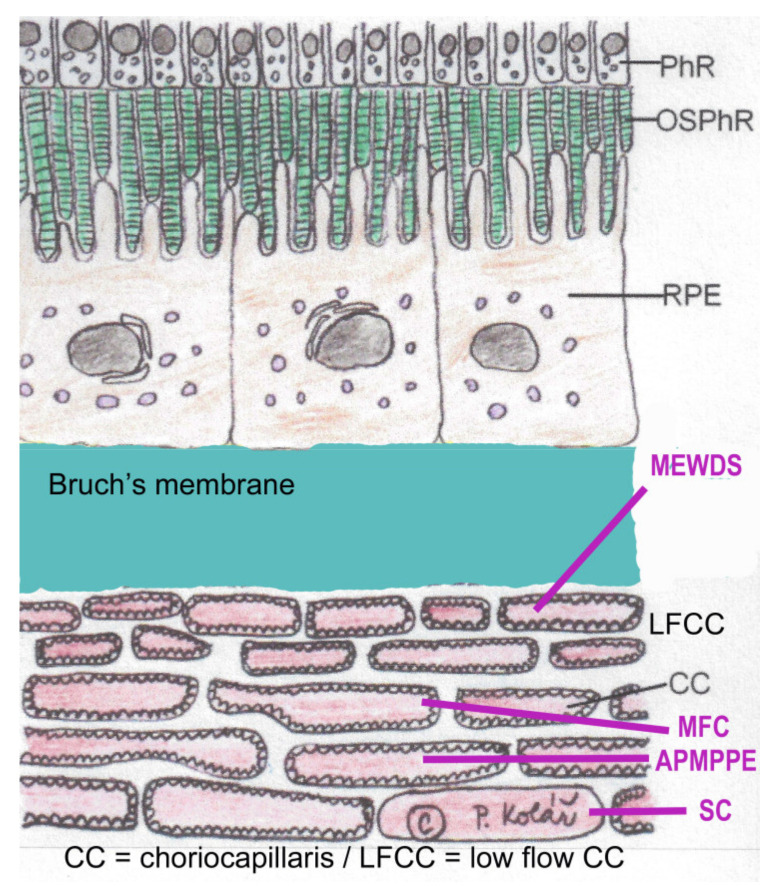
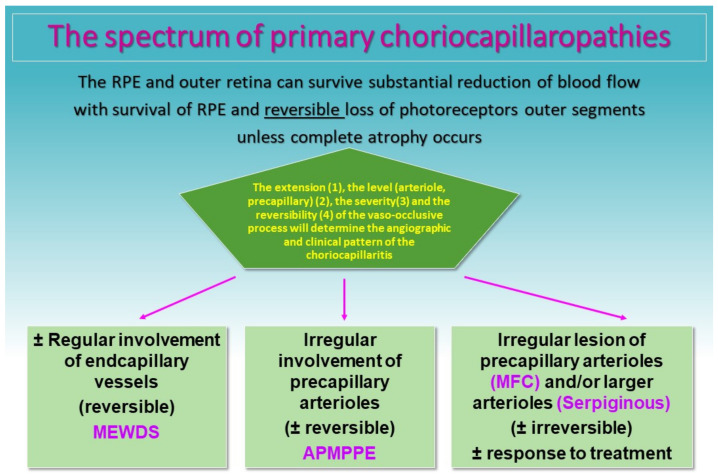
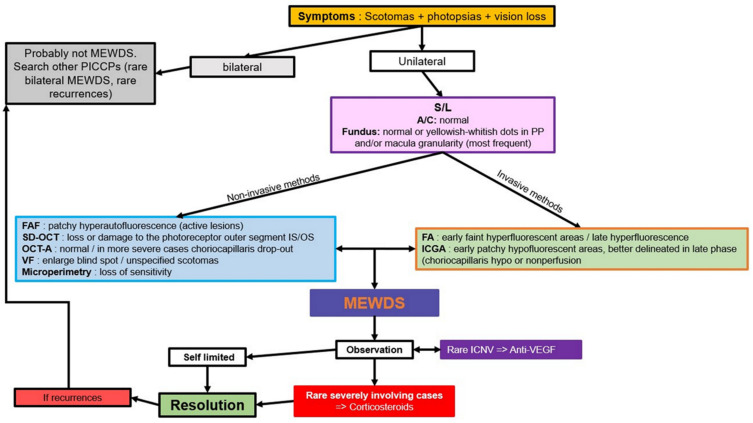
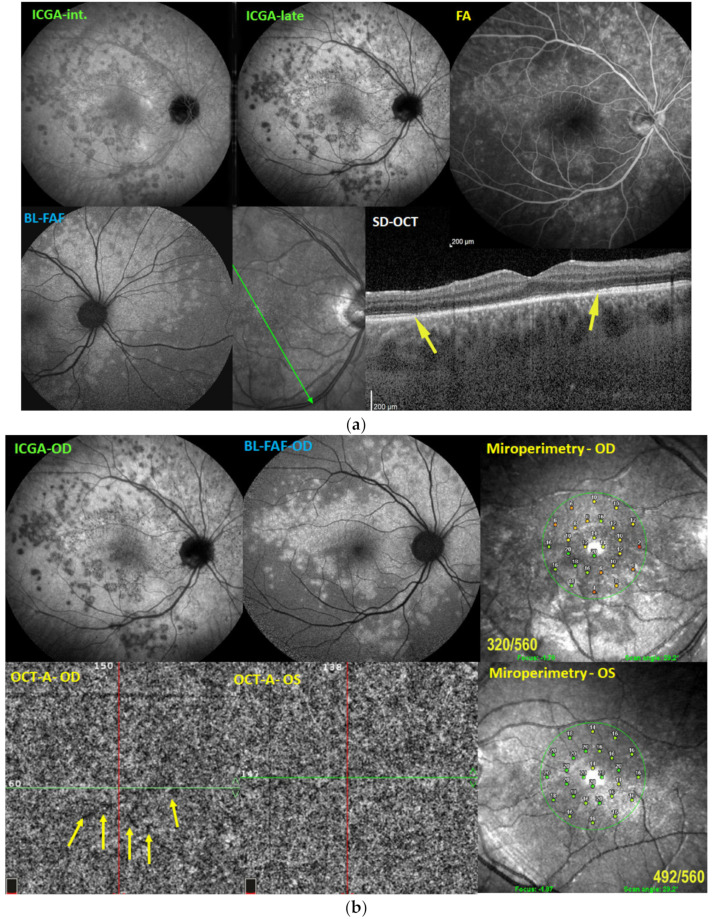
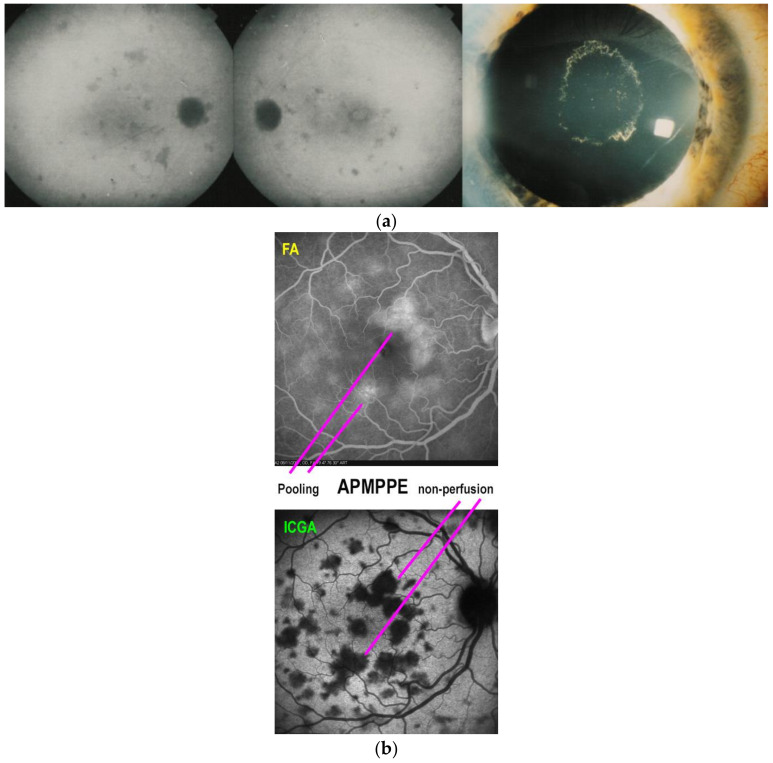
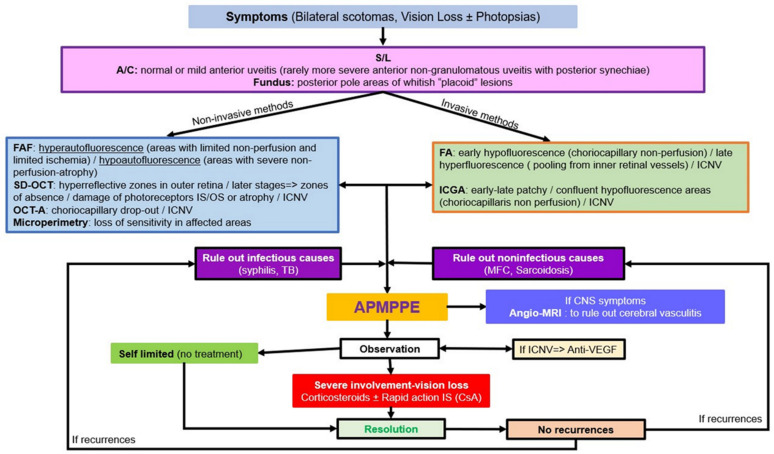
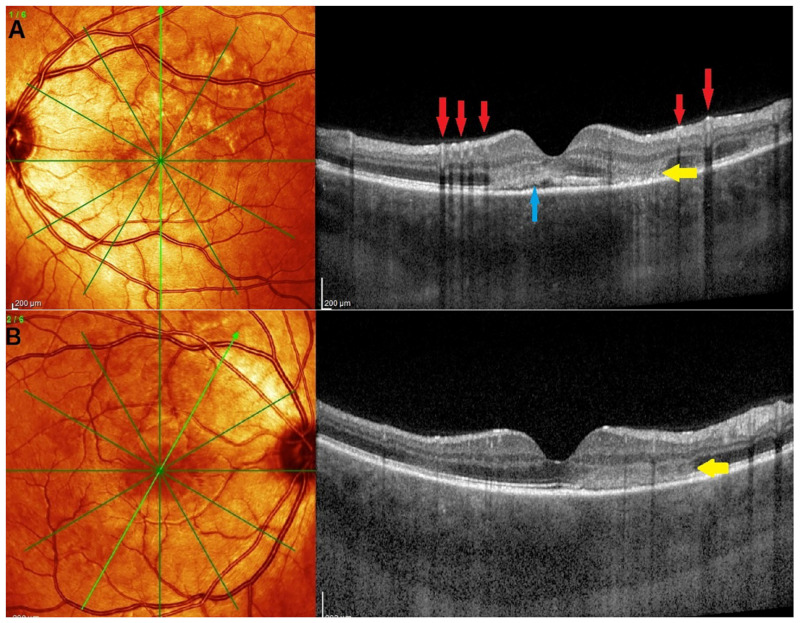
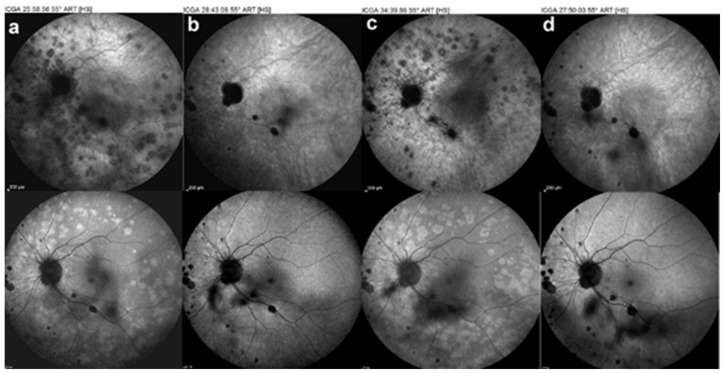
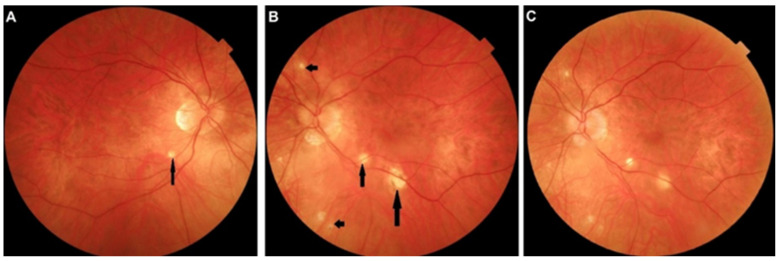
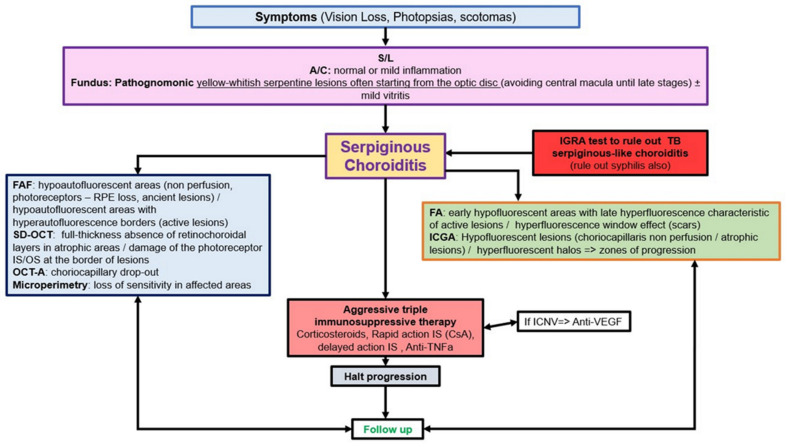
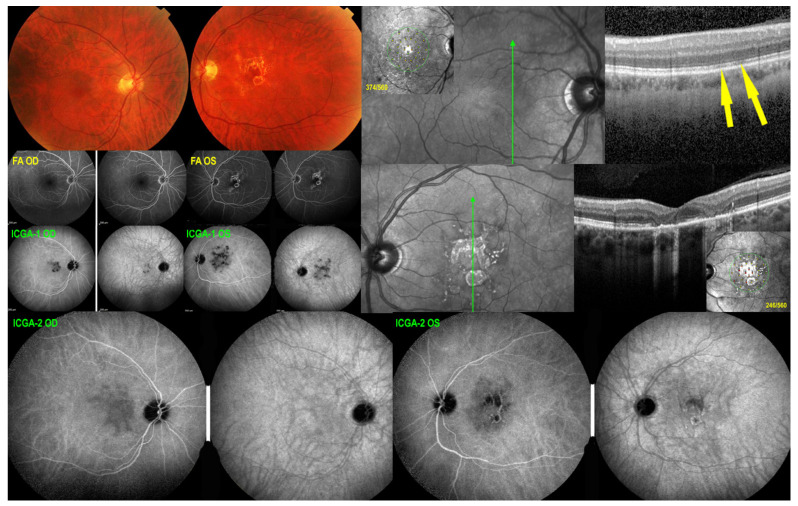
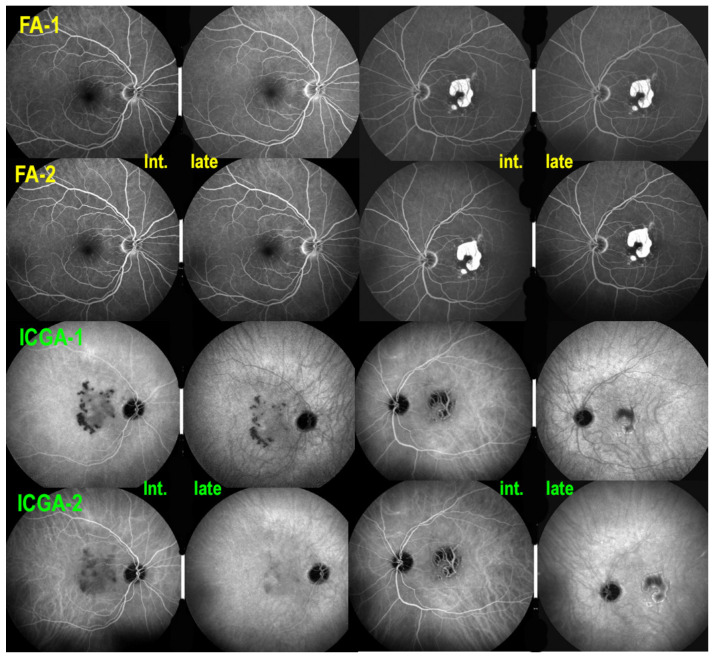
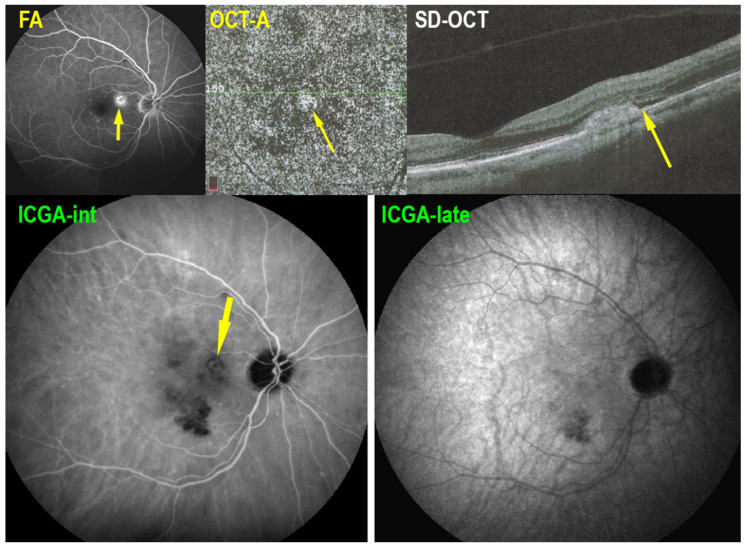
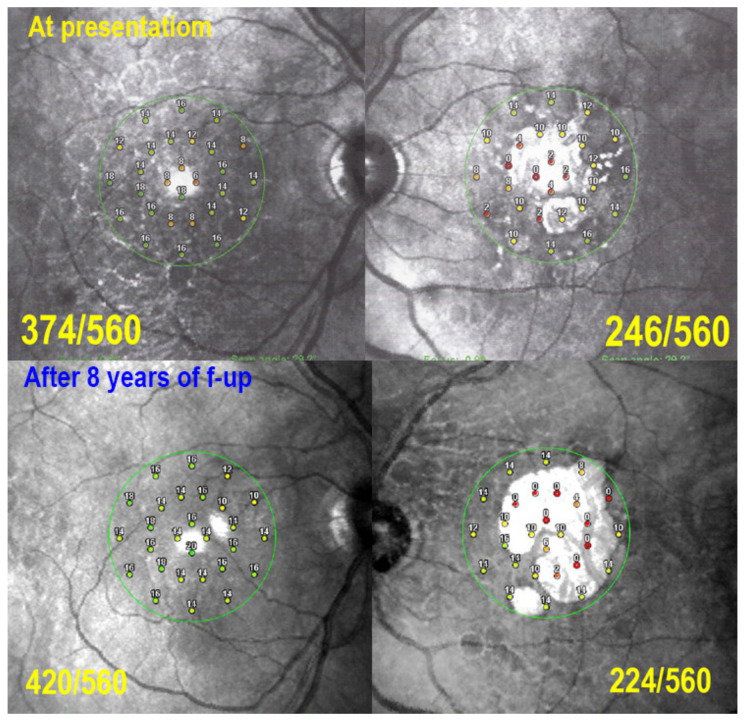
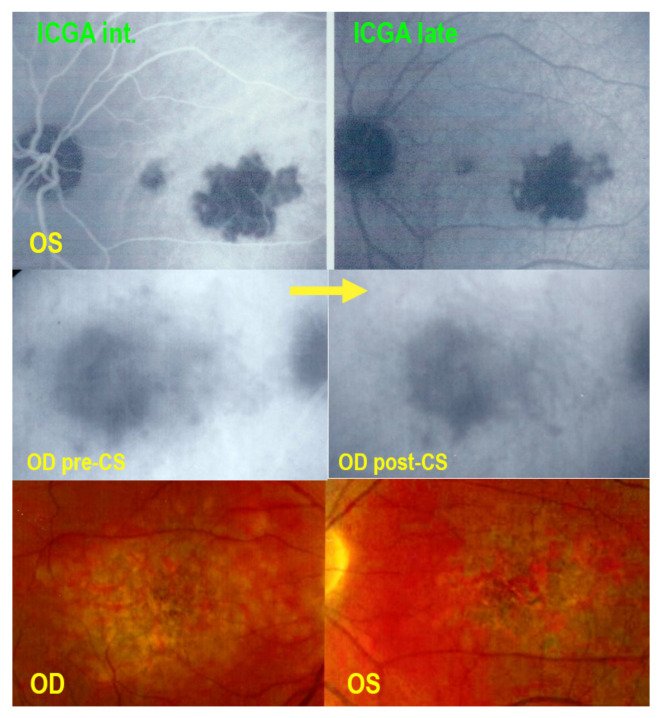
Results: Choriocapillaris non-perfusion can affect the end-choriocappilaries, at the benign end of the PICCP spectrum (MEWDS), to larger choriocapillaris vessels or precapillary vessels at the origin of more severe forms such as acute posterior multifocal placoid pigment epitheliopathy (APMPPE), idiopathic multifocal choroiditis (MFC) and Serpiginous Choroiditis (SC). Diagnosis is mostly based on multimodal imaging and especially on indocyanine green angiography (ICGA), fundus autofluorescence (FAF) and spectral-domain optical coherence tomography (SD-OCT)/OCT-angiography (OCT-A). ICGA shows the typical pattern of patchy lobular hypofluorescence reflecting hypo- or non-perfusion of the choriocapillaris that can also take the aspect of geographic areas in the more severe forms. Treatment depends on the severity of the disease and goes from observation in MEWDS and some mild cases of APMPPE, to oral corticosteroid and/or immunomodulator agents in the more severe conditions of APMPPE and MFC and SC cases. Close multimodal monitoring is crucial in order to introduce or adjust treatment.
Conclusion: PICCPs are resulting from one common clinicopathological mechanism, inflammatory choriocapillaris hypo- or non-perfusion. ICGA findings are essential for the diagnosis and follow-up of PICCPs, but non-invasive methods such as FAF and SD-OCT/OCT-A also have their role especially in follow-up of the diseases. Treatment should be individualized according to the pathology and the evolution of lesions.
Keywords: APMPPE; FA; ICGA; MEWDS; MFC; OCT-A; PICPPS; SC; SDOCT; non-infectious posterior uveitis.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Acute Posterior Multifocal Placoid Pigment Epitheliopathy (APMPPE): A Comprehensive Approach and Case Series: Systemic Corticosteroid Therapy Is Necessary in a Large Proportion of Cases.Medicina (Kaunas). 2022 Aug 8;58(8):1070. doi: 10.3390/medicina58081070. Medicina (Kaunas). 2022. PMID: 36013537 Free PMC article.
-
Diagnosis, Mechanisms, and Differentiation of Inflammatory Diseases of the Outer Retina: Photoreceptoritis versus Choriocapillaritis; A Multimodal Imaging Perspective.Diagnostics (Basel). 2022 Sep 9;12(9):2179. doi: 10.3390/diagnostics12092179. Diagnostics (Basel). 2022. PMID: 36140579 Free PMC article.
-
Review of the Current Literature and Our Experience on the Value of OCT-angiography in White Dot Syndromes.Ocul Immunol Inflamm. 2022 Feb 17;30(2):364-378. doi: 10.1080/09273948.2020.1837185. Epub 2021 Feb 22. Ocul Immunol Inflamm. 2022. PMID: 33617412 Review.
-
Choroidal perfusion abnormalities associated with Acute Posterior Multifocal Placoid Pigment Epitheliopathy: a case report.BMC Ophthalmol. 2018 Apr 10;18(1):87. doi: 10.1186/s12886-018-0756-8. BMC Ophthalmol. 2018. PMID: 29631552 Free PMC article.
-
Blue-Light Fundus Autofluorescence (BAF), an Essential Modality for the Evaluation of Inflammatory Diseases of the Photoreceptors: An Imaging Narrative.Diagnostics (Basel). 2023 Jul 24;13(14):2466. doi: 10.3390/diagnostics13142466. Diagnostics (Basel). 2023. PMID: 37510210 Free PMC article. Review.
Cited by
-
Acute Posterior Multifocal Placoid Pigment Epitheliopathy (APMPPE): A Comprehensive Approach and Case Series: Systemic Corticosteroid Therapy Is Necessary in a Large Proportion of Cases.Medicina (Kaunas). 2022 Aug 8;58(8):1070. doi: 10.3390/medicina58081070. Medicina (Kaunas). 2022. PMID: 36013537 Free PMC article.
-
Atypical Acute Ischemic Choriocapillaritis: A Case Report.Clin Case Rep. 2024 Dec 16;12(12):e9646. doi: 10.1002/ccr3.9646. eCollection 2024 Dec. Clin Case Rep. 2024. PMID: 39691487 Free PMC article.
-
Optical Coherence Tomography Angiography (OCT-A) in Uveitis: A Literature Review and a Reassessment of Its Real Role.Diagnostics (Basel). 2023 Feb 7;13(4):601. doi: 10.3390/diagnostics13040601. Diagnostics (Basel). 2023. PMID: 36832089 Free PMC article. Review.
-
Mechanisms, Pathophysiology and Current Immunomodulatory/Immunosuppressive Therapy of Non-Infectious and/or Immune-Mediated Choroiditis.Pharmaceuticals (Basel). 2022 Mar 24;15(4):398. doi: 10.3390/ph15040398. Pharmaceuticals (Basel). 2022. PMID: 35455395 Free PMC article. Review.
-
Benefits and Limitations of OCT-A in the Diagnosis and Follow-Up of Posterior Intraocular Inflammation in Current Clinical Practice: A Valuable Tool or a Deceiver?Diagnostics (Basel). 2022 Sep 30;12(10):2384. doi: 10.3390/diagnostics12102384. Diagnostics (Basel). 2022. PMID: 36292075 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
