

Independent Association of Lipoprotein(a) and Coronary Artery Calcification With Atherosclerotic Cardiovascular Risk
- PMID: 35210030
- PMCID: PMC10966924
- DOI: 10.1016/j.jacc.2021.11.058
Independent Association of Lipoprotein(a) and Coronary Artery Calcification With Atherosclerotic Cardiovascular Risk
Abstract
Background: Elevated lipoprotein(a) [Lp(a)] and coronary artery calcium (CAC) score are individually associated with increased atherosclerotic cardiovascular disease (ASCVD) risk but have not been studied in combination.
Objectives: This study sought to investigate the independent and joint association of Lp(a) and CAC with ASCVD risk.
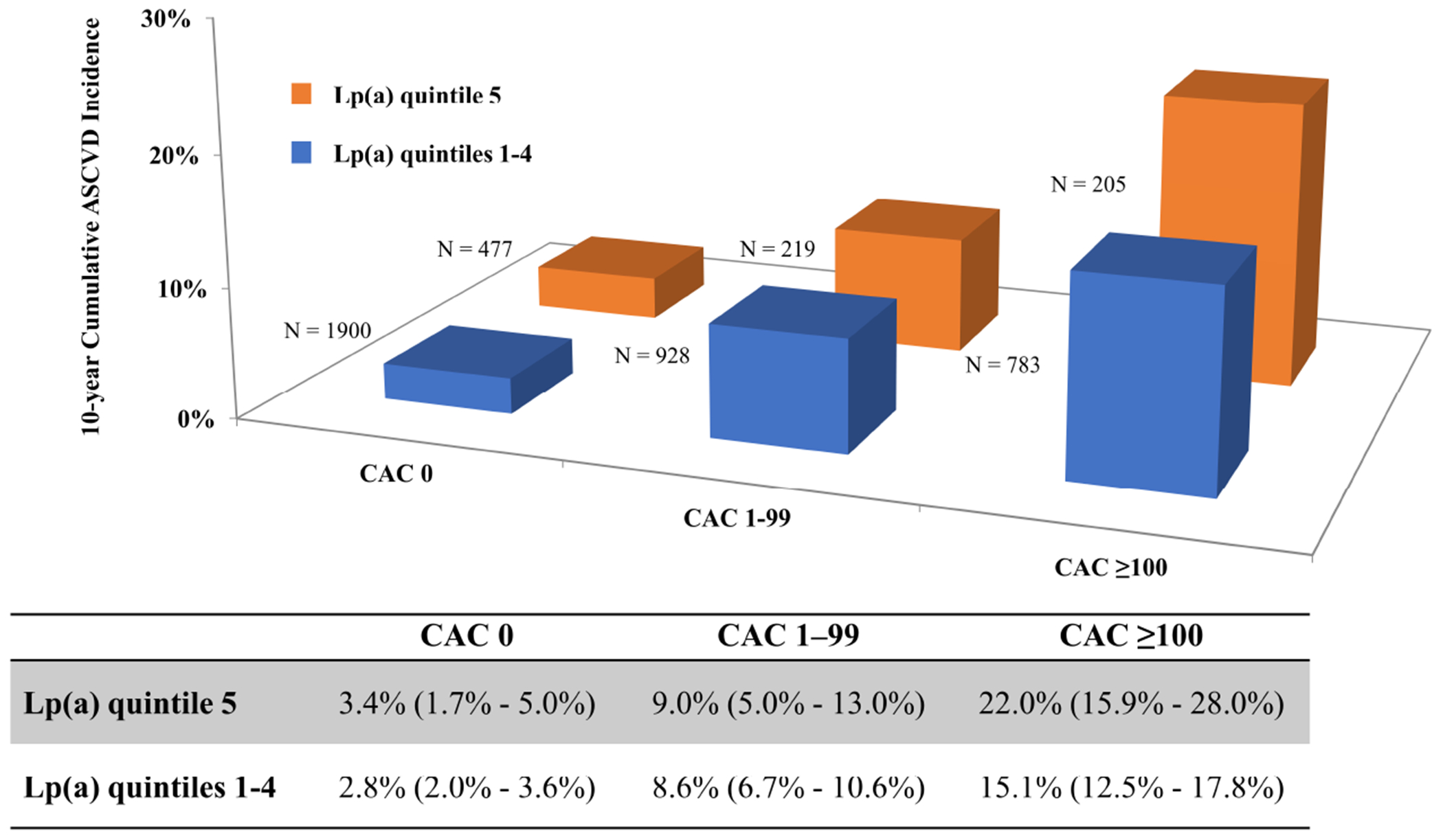
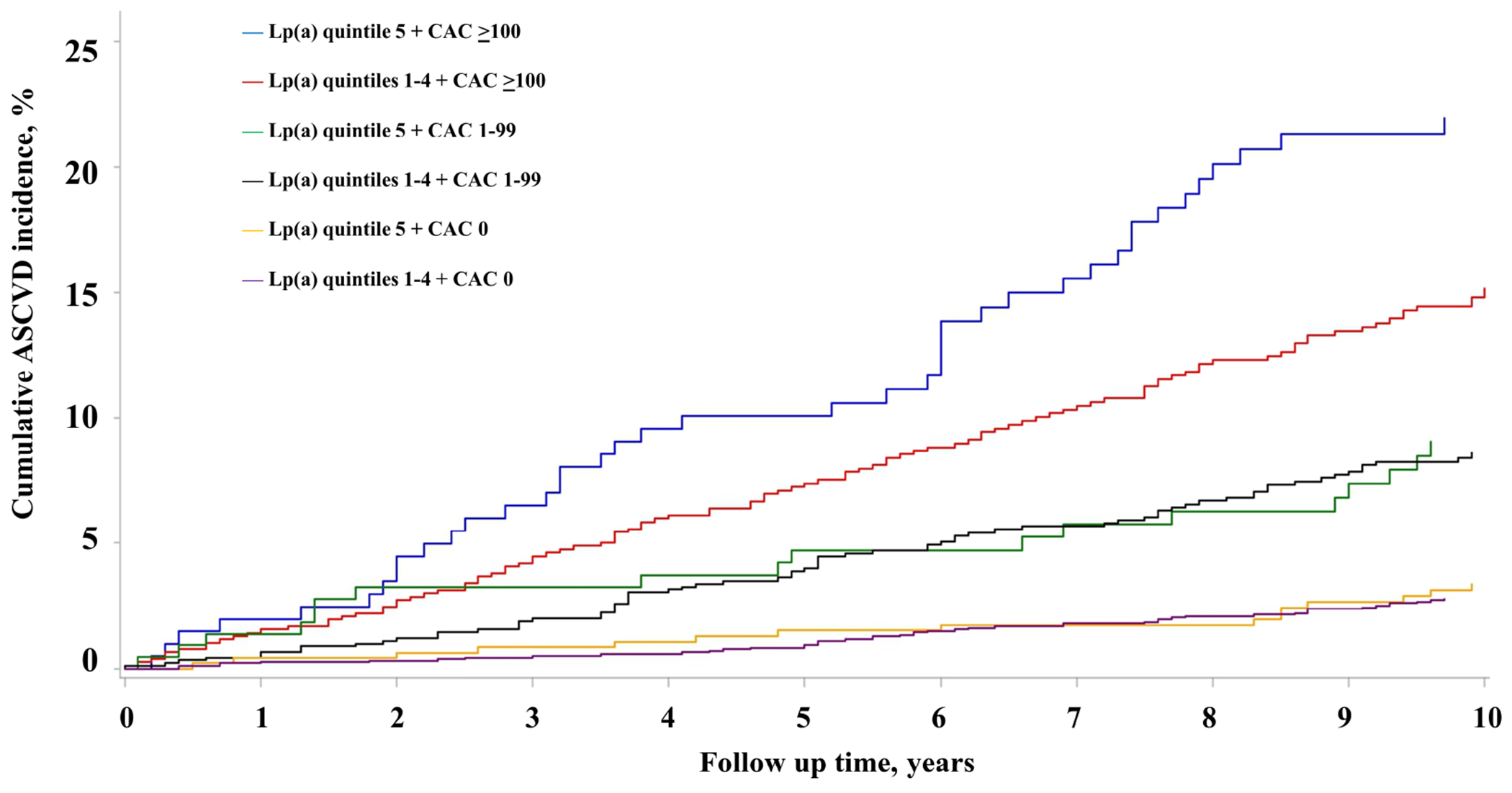
Methods: Plasma Lp(a) and CAC were measured at enrollment among asymptomatic participants of the MESA (Multi-Ethnic Study of Atherosclerosis) (n = 4,512) and DHS (Dallas Heart Study) (n = 2,078) cohorts. Elevated Lp(a) was defined as the highest race-specific quintile, and 3 CAC score categories were studied (0, 1-99, and ≥100). Associations of Lp(a) and CAC with ASCVD risk were evaluated using risk factor-adjusted Cox regression models.
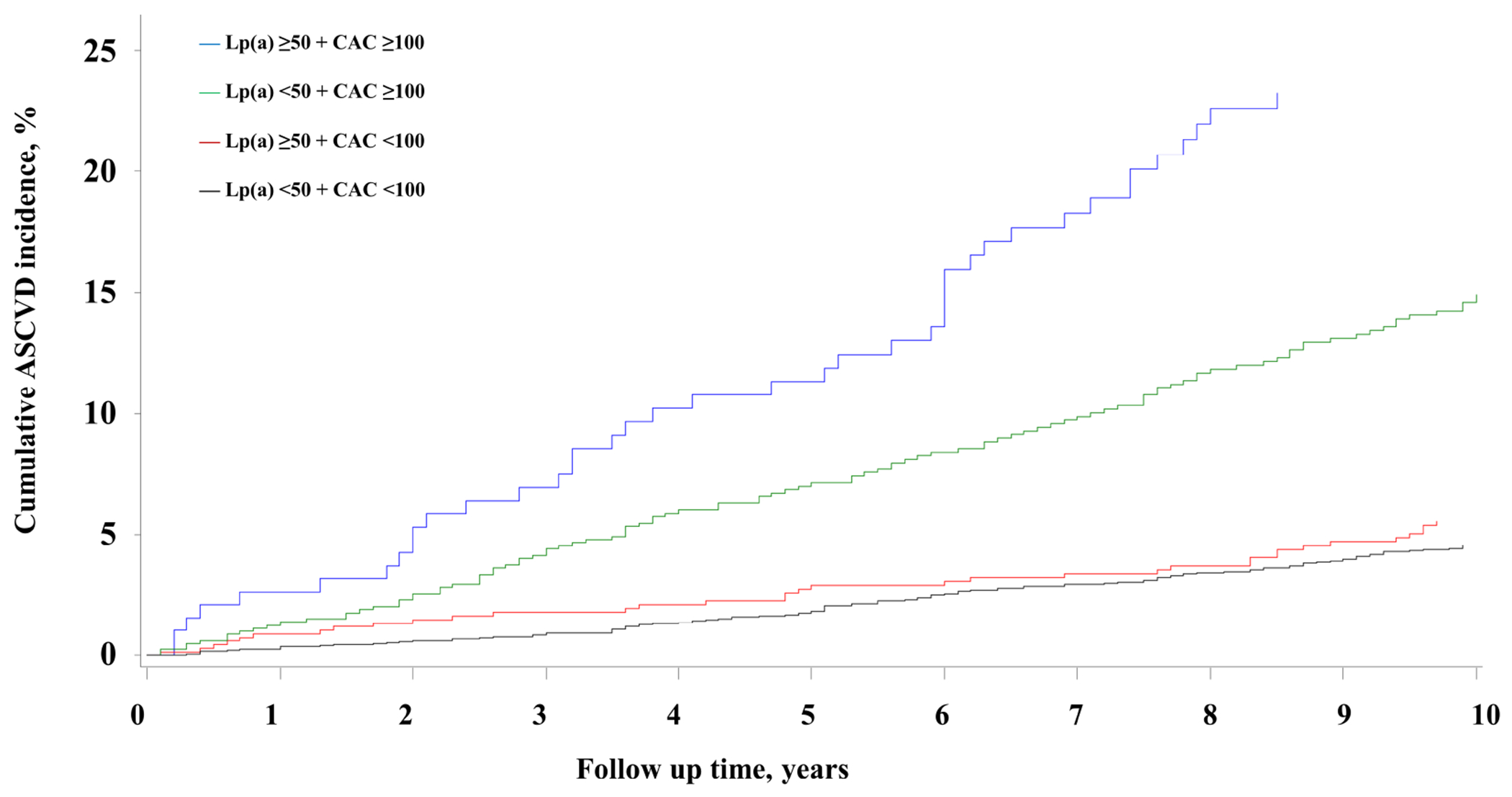
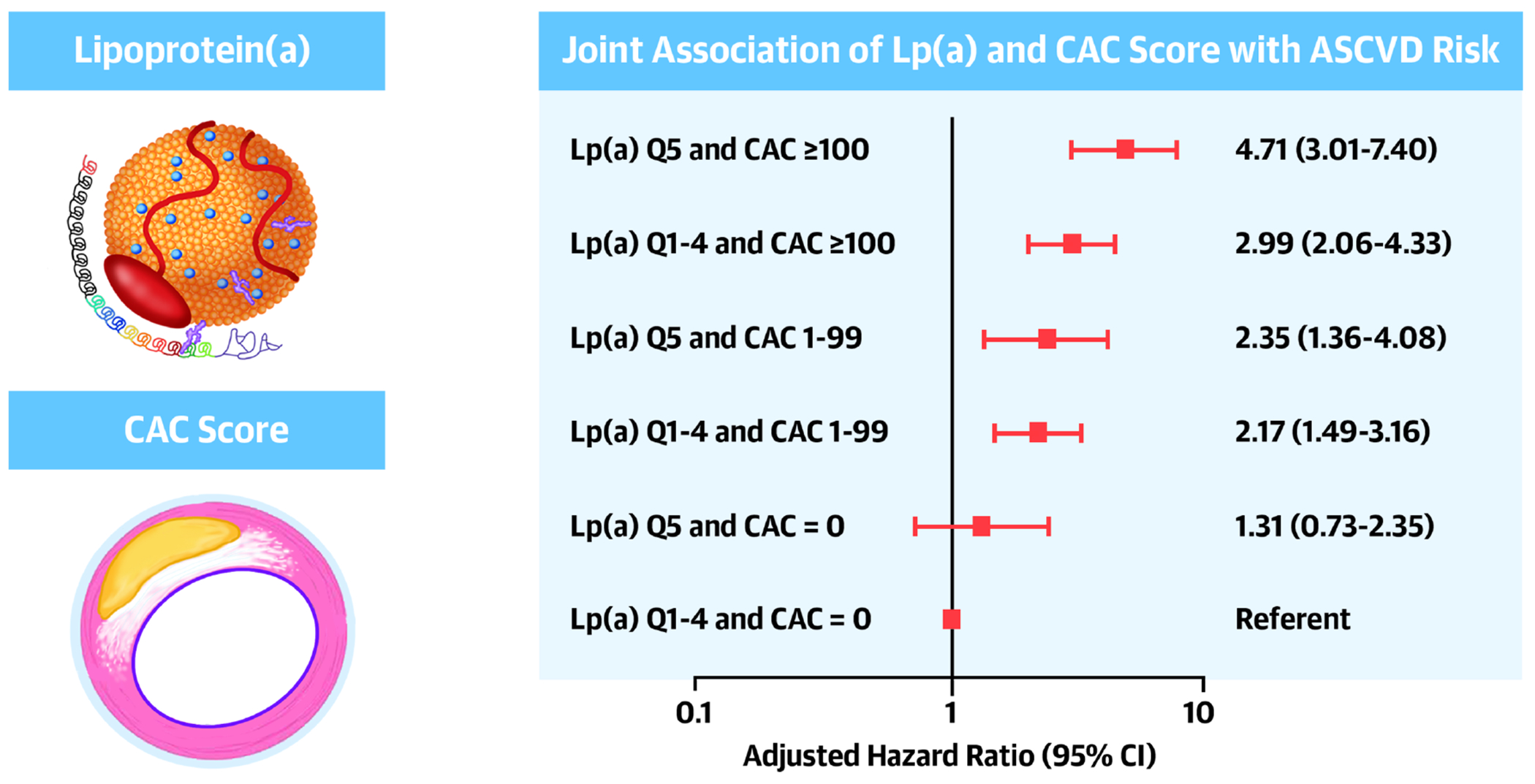
Results: Among MESA participants (61.9 years of age, 52.5% women, 36.8% White, 29.3% Black, 22.2% Hispanic, and 11.7% Chinese), 476 incident ASCVD events were observed during 13.2 years of follow-up. Elevated Lp(a) and CAC score (1-99 and ≥100) were independently associated with ASCVD risk (HR: 1.29; 95% CI: 1.04-1.61; HR: 1.68; 95% CI: 1.30-2.16; and HR: 2.66; 95% CI: 2.07-3.43, respectively), and Lp(a)-by-CAC interaction was not noted. Compared with participants with nonelevated Lp(a) and CAC = 0, those with elevated Lp(a) and CAC ≥100 were at the highest risk (HR: 4.71; 95% CI: 3.01-7.40), and those with elevated Lp(a) and CAC = 0 were at a similar risk (HR: 1.31; 95% CI: 0.73-2.35). Similar findings were observed when guideline-recommended Lp(a) and CAC thresholds were considered, and findings were replicated in the DHS.
Conclusions: Lp(a) and CAC are independently associated with ASCVD risk and may be useful concurrently for guiding primary prevention therapy decisions.
Keywords: atherosclerotic cardiovascular disease; coronary artery calcium; lipoprotein(a); primary cardiovascular disease prevention.
Copyright © 2022 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Funding Support and Author Disclosures The MESA study is supported by contracts 75N92020D00001, HHSN268201500003I, N01-HC-95159, 75N92020D00005, N01-HC-95160, 75N92020D00002, N01-HC-95161, 75N92020D00003, N01-HC-95162, 75N92020D00006, N01-HC-95163, 75N92020D00004, N01-HC-95164, 75N92020D00007, N01-HC-95165, N01-HC-95166, N01-HC-95167, N01-HC-95168, and N01-HC-95169 from the National Heart, Lung, and Blood Institute; and by grants UL1-TR-000040, UL1-TR-001079, and UL1-TR-001420 from the National Center for Advancing Translational Sciences. The DHS study was funded by the Donald W. Reynolds Foundation, Las Vegas, Nevada, and partially supported by the National Center for Advancing Translational Sciences of the National Institutes of Health under award number UL1TR001105. Dr Virani has received grant support from the Department of Veterans Affairs, the World Heart Federation, and the Tahir and Jooma Family; has received honorarium from American College of Cardiology (Associate Editor for Innovations, acc.org). Dr Joshi has received grant support from the American Heart Association, NASA, and Novo Nordisk; has received consulting income from Bayer and Regeneron; owns equity in G3 Therapeutics; and has served as a site investigator with all funds to the institution from GlaxoSmithKline, Sanofi, AstraZeneca, and Novartis. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
Comment in
-
Lipoprotein(a) and Coronary Calcium: Clinical Management and Potential Design of Primary Prevention Trials.J Am Coll Cardiol. 2022 Mar 1;79(8):769-771. doi: 10.1016/j.jacc.2021.12.018. J Am Coll Cardiol. 2022. PMID: 35210031 No abstract available.
-
Accuracy Transcends Simplicity in Coronary Atherosclerosis Imaging.J Am Coll Cardiol. 2022 Jun 21;79(24):e487. doi: 10.1016/j.jacc.2022.03.386. J Am Coll Cardiol. 2022. PMID: 35710198 No abstract available.
-
Reply: Accuracy Transcends Simplicity in Coronary Atherosclerosis Imaging.J Am Coll Cardiol. 2022 Jun 21;79(24):e489. doi: 10.1016/j.jacc.2022.04.018. J Am Coll Cardiol. 2022. PMID: 35710199 No abstract available.
References
-
- Tsimikas S. A Test in Context: Lipoprotein(a): Diagnosis, Prognosis, Controversies, and Emerging Therapies. J Am Coll Cardiol 2017;69:692–711. - PubMed
-
- Kamstrup PR, Tybjaerg-Hansen A, Nordestgaard BG. Extreme lipoprotein(a) levels and improved cardiovascular risk prediction. J Am Coll Cardiol 2013;61:1146–56. - PubMed
-
- Clarke R, Peden JF, Hopewell JC et al. Genetic variants associated with Lp(a) lipoprotein level and coronary disease. N Engl J Med 2009;361:2518–28. - PubMed
-
- Agatston AS, Janowitz WR, Hildner FJ, Zusmer NR, Viamonte M Jr., Detrano R. Quantification of coronary artery calcium using ultrafast computed tomography. J Am Coll Cardiol 1990;15:827–32. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- N01 HC095168/HL/NHLBI NIH HHS/United States
- UL1 TR001105/TR/NCATS NIH HHS/United States
- 75N92020D00001/HL/NHLBI NIH HHS/United States
- N01 HC095167/HL/NHLBI NIH HHS/United States
- HHSN268201500003I/HL/NHLBI NIH HHS/United States
- UL1 TR000040/TR/NCATS NIH HHS/United States
- N01 HC095166/HL/NHLBI NIH HHS/United States
- N01 HC095160/HL/NHLBI NIH HHS/United States
- 75N92020D00002/HL/NHLBI NIH HHS/United States
- HHSN268201500003C/HL/NHLBI NIH HHS/United States
- N01 HC095161/HL/NHLBI NIH HHS/United States
- 75N92020D00005/HL/NHLBI NIH HHS/United States
- UL1 TR001079/TR/NCATS NIH HHS/United States
- N01 HC095169/HL/NHLBI NIH HHS/United States
- N01 HC095159/HL/NHLBI NIH HHS/United States
- 75N92020D00003/HL/NHLBI NIH HHS/United States
- UL1 TR001420/TR/NCATS NIH HHS/United States
- 75N92020D00004/HL/NHLBI NIH HHS/United States
- N01 HC095163/HL/NHLBI NIH HHS/United States
- 75N92020D00007/HL/NHLBI NIH HHS/United States
- N01 HC095162/HL/NHLBI NIH HHS/United States
- 75N92020D00006/HL/NHLBI NIH HHS/United States
- N01 HC095165/HL/NHLBI NIH HHS/United States
- N01 HC095164/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
