

Asthma management in low and middle income countries: case for change
- PMID: 35210321
- PMCID: PMC9474897
- DOI: 10.1183/13993003.03179-2021
Asthma management in low and middle income countries: case for change
Abstract
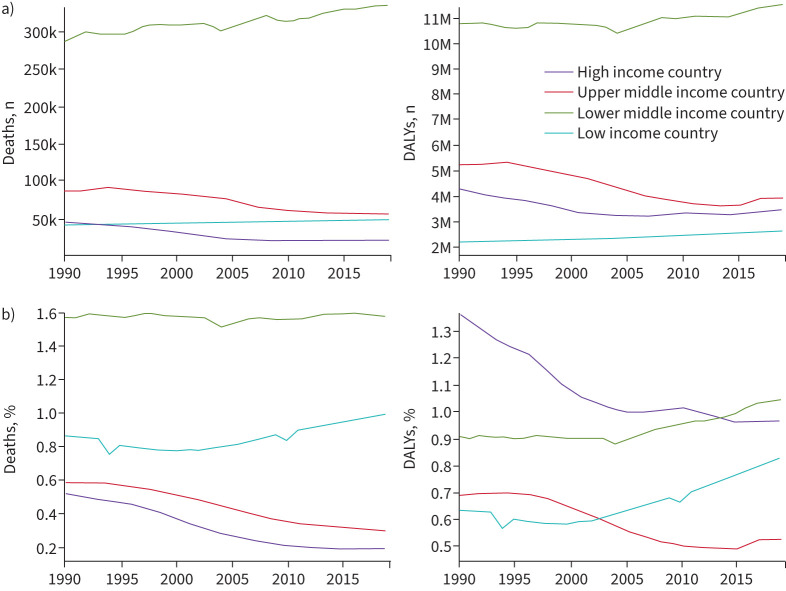
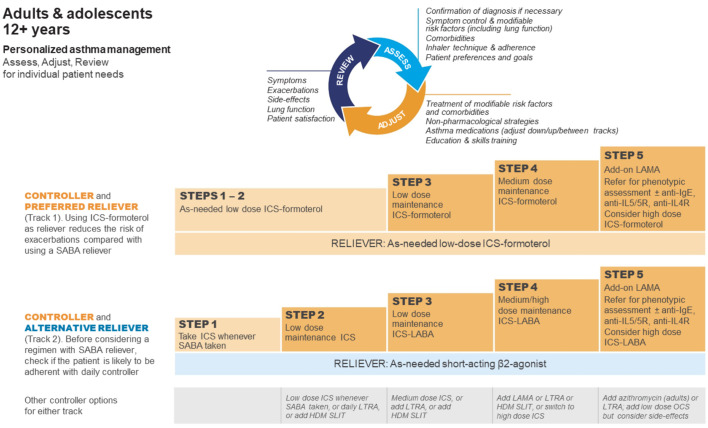
Asthma is the most common noncommunicable disease in children, and among the most common in adults. The great majority of people with asthma live in low and middle income countries (LMICs), which have disproportionately high asthma-related morbidity and mortality. Essential inhaled medications, particularly those containing inhaled corticosteroids (ICS), are often unavailable or unaffordable, and this explains much of the global burden of preventable asthma morbidity and mortality. Guidelines developed for LMICs are generally based on the outdated assumption that patients with asthma symptoms <1-3 times per week do not need (or benefit from) ICS. Even when ICS are prescribed, many patients manage their asthma with oral or inhaled short-acting β2-agonists (SABA) alone, owing to issues of availability and affordability. A single ICS-formoterol inhaler-based approach to asthma management for all severities of asthma, from mild to severe, starting at diagnosis, might overcome SABA overuse/over-reliance and reduce the burden of symptoms and severe exacerbations. However, ICS-formoterol inhalers are currently very poorly available or unaffordable in LMICs. There is a pressing need for pragmatic clinical trial evidence of the feasibility and cost-effectiveness of this and other strategies to improve asthma care in these countries. The global health inequality in asthma care that deprives so many children, adolescents and adults of healthy lives and puts them at increased risk of death, despite the availability of highly effective therapeutic approaches, is unacceptable. A World Health Assembly Resolution on universal access to affordable and effective asthma care is needed to focus attention and investment on addressing this need.
Copyright ©The authors 2022.
Conflict of interest statement
Conflict of interest: The Global Initiative for Asthma (GINA) provided writing assistance during the course of the present manuscript. K. Mortimer additionally reports consulting fees from AstraZeneca, outside the submitted work, and is a member of the science committee for GINA. H.K. Reddel reports grants from AstraZeneca, GlaxoSmithKline and Novartis; consulting fees from Novartis; lecture honoraria from AstraZeneca, GlaxoSmithKline, Teva, Boehringer Ingelheim, Sanofi and Chiesi; and participation on advisory boards for AstraZeneca, GlaxoSmithKline, Novartis, Chiesi and Sanofi, outside the submitted work; and is also Chair of Scientific Committee and Member of Board of Directors for GINA, and Member of Australian Asthma Guidelines Committee for National Asthma Council. P.M. Pitrez reports consulting fees from AstraZeneca, Novartis, GSK, Boehringer Ingelheim and Sanofi; lecture honoraria from AstraZeneca, Novartis, GSK, Boehringer Ingelheim and Sanofi; and travel support from GSK and Boehringer Ingelheim, outside the submitted work. E.D. Bateman reports consulting fees from AstraZeneca, Sanofi Genzyme, Regeneron, Novartis and ALK; and lecture honoraria from AstraZeneca, Orion, Menarini, Novartis, Sanofi Genzyme and Regeneron, outside the submitted work; and is also a member of the Board and Science Committee of GINA.
Figures
References
-
- Global Asthma Network . The Global Asthma Report 2018. Auckland, Global Asthma Network, 2018.
-
- Global Burden of Disease 2019 Diseases and Injuries Collaborators . Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020; 396: 1204–1222. doi: 10.1016/S0140-6736(20)30925-9 - DOI - PMC - PubMed