

T2-high asthma phenotypes across lifespan
- PMID: 35210326
- PMCID: PMC9520028
- DOI: 10.1183/13993003.02288-2021
T2-high asthma phenotypes across lifespan
Abstract
Rationale: In adults, personalised asthma treatment targets patients with type 2 (T2)-high and eosinophilic asthma phenotypes. It is unclear whether such classification is achievable in children.
Objectives: To define T2-high asthma with easily accessible biomarkers and compare resulting phenotypes across all ages.
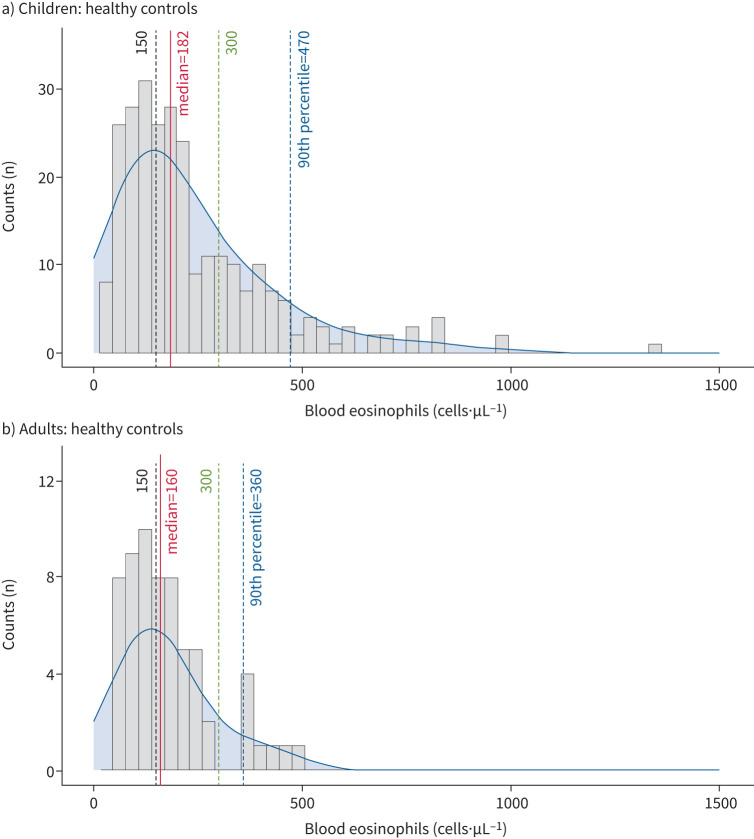
Methods: In the multicentre clinical All Age Asthma Cohort (ALLIANCE), 1125 participants (n=776 asthmatics, n=349 controls) were recruited and followed for 2 years (1 year in adults). Extensive clinical characterisation (questionnaires, blood differential count, allergy testing, lung function and sputum induction (in adults)) was performed at baseline and follow-ups. Interleukin (IL)-4, IL-5 and IL-13 were measured after stimulation of whole blood with lipopolysaccharide (LPS) or anti-CD3/CD28.
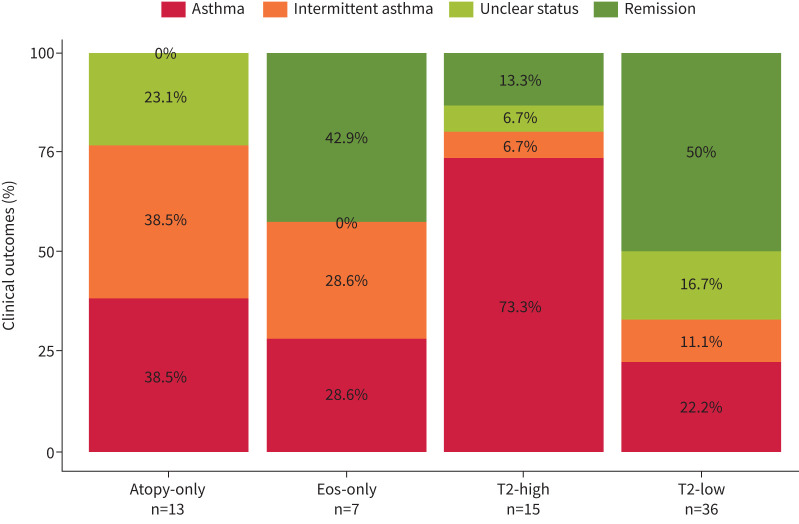
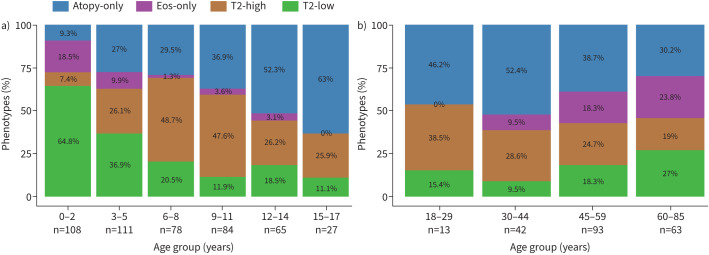
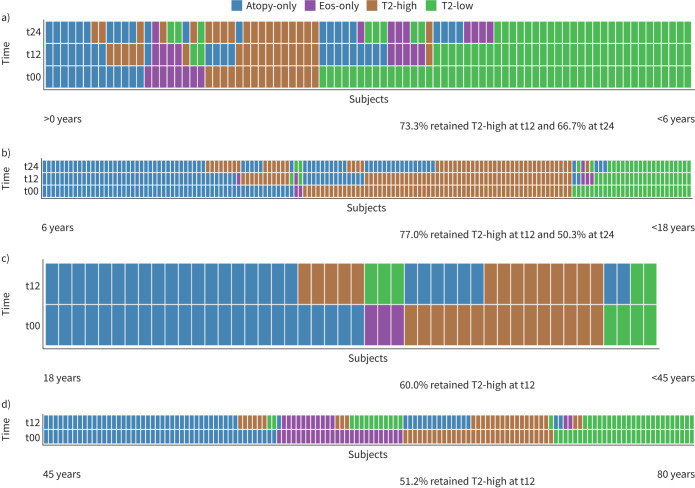
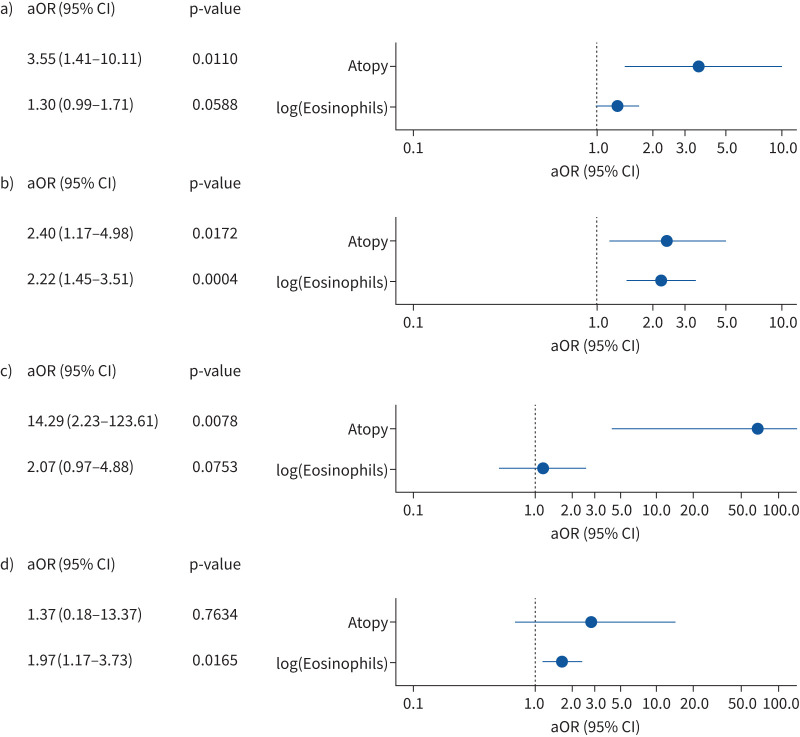
Measurements and main results: Based on blood eosinophil counts and allergen-specific serum IgE antibodies, patients were categorised into four mutually exclusive phenotypes: "atopy-only", "eosinophils-only", "T2-high" (eosinophilia + atopy) and "T2-low" (neither eosinophilia nor atopy). The T2-high phenotype was found across all ages, even in very young children in whom it persisted to a large degree even after 2 years of follow-up. T2-high asthma in adults was associated with childhood onset, suggesting early origins of this asthma phenotype. In both children and adults, the T2-high phenotype was characterised by excessive production of specific IgE to allergens (p<0.0001) and, from school age onwards, by increased production of IL-5 after anti-CD3/CD28 stimulation of whole blood.
Conclusions: Using easily accessible biomarkers, patients with T2-high asthma can be identified across all ages delineating a distinct phenotype. These patients may benefit from therapy with biologicals even at a younger age.
Trial registration: ClinicalTrials.gov NCT02496468 NCT02419274.
Copyright ©The authors 2022.
Conflict of interest statement
Conflict of interest: N. Maison, J. Omony, S. Illi, D. Thiele, A.M. Dittrich, C. Happle, M. Meyer, S. Foth and R. Grychtol have nothing to disclose. C. Skevaki reports grants and personal fees from Hycor Biomedical, Bencard Allergie, Thermo Fisher Scientific as well as grants from Mead Johnson Nutrition (MJN), Universities Giessen and Marburg Lung Centre, the German Centre for Lung Research (DZL), University Hospital Giessen and Marburg, Deutsche Forschungsgemeinschaft (DFG). T. Bahmer reports grants from the Federal Ministry for Education and Research (BMBF) for the German Center for Lung Research (DZL) and personal fees from AstraZeneca, GlaxoSmithKline, Novartis, Roche and Chiesi. M. Weckmann reports grants from Federal Ministry for Education and Research (BMBF), University of Luebeck and German Academic Exchange Service. B. Schaub reports grants from DFG, BMBF, the EU as well from GlaxoSmithKline, Sanofi and Novartis. H. Renz reports grants from German Center for Lung Disease (DZL) and Universities Giessen Marburg Lung Center. M.V. Kopp reports grants and personal fees from Allergopharma GmbH and Vertex GmbH; additional, personal fees from Sanofi GmbH, Infectopharm GmbH and Leti GmbH. E. Rietschel reports personal lecture payments for Nutricia Milupa GmbH and Novartis Pharma, and honoraria for participation in advisory boards for MICE-Mylan, Novartis Pharma GmbH and Boehringer Ingelheim GmbH. K.F. Rabe recieved personal payments or honoraria from AstraZeneca, Boehringer Ingelheim, Chiesi Pharmaceuticals, Novartis, Sanofi & Regeneron, GlaxoSmithKline, Berlin Chemie and Roche; K.F. Rabe also discloses participation on data safety monitoring boards/advisory boards for AstraZeneca and Sanofi Regeneron, and leadership or fiduciary role in the German Center for Lung Research (DZL), German Chest Society (DGP) and American Thoracic Society (ATS). G. Hansen reports grants from German Federal Ministry of Education and Research (BMBF) and German Research Foundation (DFG) as well as personal fees from Sanofi GmbH, MedUpdate, and Abbvie. E. von Mutius reports grants from the German Center for Lung Research (DZL) as well as royalties/licenses held by Elsevier GmbH, Gerog Thieme Verlag, Springer Verlag GmbH, Elsevier Ltd; furthermore, consultation fees were received from the Chinese University of Hong Kong, European Commission, HiPP GmbH and AstraZeneca; E. von Mutius also received payments and/or support for meetings/travel from the Massachusetts Medical Society, Springer-Verlag GmbH, Elsevier Ltd, Böhringer Ingelheim International GmbH, European Respiratory Society (ERS), University Utrecht, Salzburg, Colorado and Imperial College London, Springer Medizin Verlag GmbH, Japanese Society of Pediatric Allergy and Clinical Immunology, Klinkum Rechts der Isar, Paul-Martini-Stiftung; further support for meetings/travel was granted by Verein zur Förderung der Pneumologie am Krankenhaus Groshansdorf, Pneumologie Development Mondial Congress & Events GmbH, American Academy of Allergy, Asthma & Immunology, Margaux Orange, Volkswagen Stiftung, Österreichische Gesellschaft für Allergologie & Immunologie, OM Pharma SA, Hanson Wade Ltd, iKOMM GmbH, DSI Dansk Bornestma Center, American Thoracic Society, HiPP GmbH; E. von Mutius has patent EP2361632, EP1411977, EP1637147 and EP 1964570 (licensed to Protectimmun), furthermore patent LU101064 is pending; E. von Mutius participates in the following data monitoring or advisory boards: EXPANSE, BEAMS External Scientific Advisory Board, Journal of Allergy and Clinical Immunology: in Practice, Children's Respiratory and Environmental Workgroup (CREW), International Scientific & Societal Advisory Board of Utrecht Life Sciences, External Review Panel of the Faculty of Veterinary Science (University of Utrecht), Gottfried Wilhelm Leibniz Programme, Asthma UK for Applied Research, Advisory Board of The Lancet Respiratory Medicine, CHILD (Canadian Healthy Infant Longitudinal Development Study).
Figures
Comment in
-
Moving the dial on identifying endotypes of asthma from early life.Eur Respir J. 2022 Sep 29;60(3):2201031. doi: 10.1183/13993003.01031-2022. Print 2022 Sep. Eur Respir J. 2022. PMID: 36175027 No abstract available.
References
-
- Agache I, Beltran J, Akdis C, et al. Efficacy and safety of treatment with biologicals (benralizumab, dupilumab, mepolizumab, omalizumab and reslizumab) for severe eosinophilic asthma. A systematic review for the EAACI Guidelines – recommendations on the use of biologicals in severe asthma. Allergy 2020; 75: 1023–1042. doi: 10.1111/all.14221 - DOI - PubMed