

A Novel MRI and Clinical-Based Scoring System to Assess Post-Surgery Healing and to Predict Long-Term Healing in Cryptoglandular Anal Fistulas
- PMID: 35210804
- PMCID: PMC8860728
- DOI: 10.2147/CEG.S343254
A Novel MRI and Clinical-Based Scoring System to Assess Post-Surgery Healing and to Predict Long-Term Healing in Cryptoglandular Anal Fistulas
Abstract
Background: Anal fistulas cause great uncertainty and anxiety in patients and surgeons alike. This is largely because of the inability to accurately confirm postoperative fistula healing, especially long-term healing. There is no scoring system available that can objectively assess cryptoglandular anal fistulas for postoperative healing and can also accurately predict long-term healing.
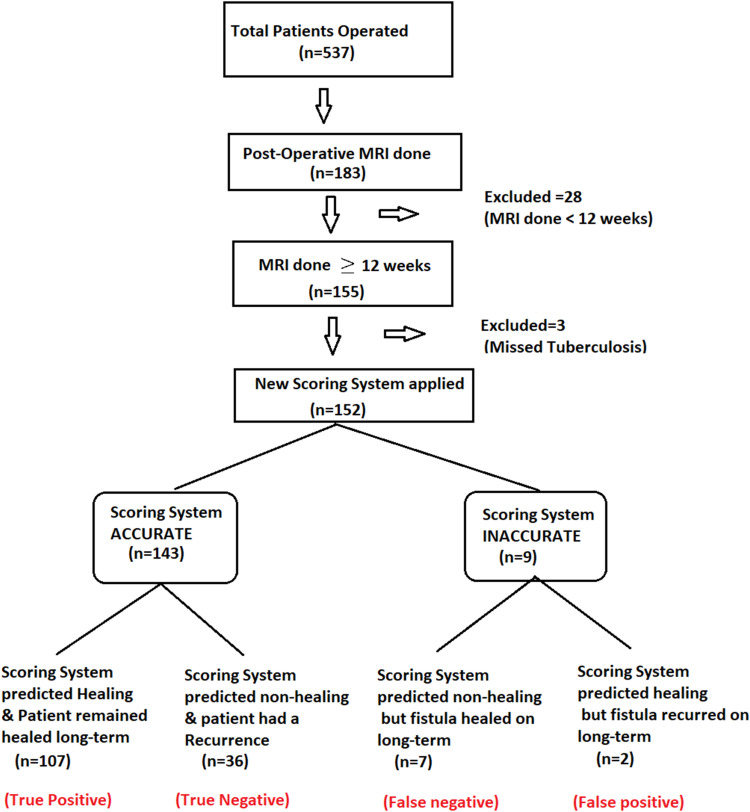
Methods: Several parameters that could indicate anal fistula healing were assessed. Out of these, six parameters (four MRI-based and two clinical) were finalized, and a weighted score was given to each parameter. A novel scoring system (NSS) was developed. A minimum possible score (zero) indicated complete healing whereas the maximum weighted score (n = 20) indicated confirmed non-healing. Scoring was done with postoperative MRI (at least 3 months post-surgery), then compared with the actual healing status, and subsequently correlated with the final long-term clinical outcome.
Results: The NSS was validated in 183 operated cryptoglandular fistula-in-ano patients over a 3-year period in whom 283 MRIs (preoperative plus postoperative) were performed. The postoperative follow-up was 12-48 months (median-30 months). The NSS was found to have a very high positive predictive value (98.2%) and moderately high negative predictive value (83.7%) for long-term fistula healing. Additionally, its sensitivity and specificity in predicting healing were 93.9% and 94.7%, respectively.
Conclusion: Thus, this new scoring system is highly accurate and would be a useful tool for surgeons and radiologists managing anal fistulas. By objectivizing the assessment of postoperative healing, it can both ease and streamline management. Moreover, reliable prediction of recurrence-free long-term healing will greatly allay the apprehensions associated with this dreaded disease.
Keywords: MRI; anal fistula; healing; internal opening; postoperative; scoring system.
© 2022 Garg et al.
Conflict of interest statement
The authors report no conflicts of interest in this work.
Figures





References
-
- Jayne DG, Scholefield J, Tolan D, et al. A multicenter randomized controlled trial comparing safety, efficacy, and cost-effectiveness of the surgisis anal fistula plug versus surgeon’s preference for transsphincteric fistula-in-ano. Ann Surg. 2021;273(3):433–441. doi: 10.1097/SLA.0000000000003981 - DOI - PubMed
LinkOut - more resources
Full Text Sources
