

Admission Random Blood Glucose, Fasting Blood Glucose, Stress Hyperglycemia Ratio, and Functional Outcomes in Patients With Acute Ischemic Stroke Treated With Intravenous Thrombolysis
- PMID: 35211004
- PMCID: PMC8861349
- DOI: 10.3389/fnagi.2022.782282
Admission Random Blood Glucose, Fasting Blood Glucose, Stress Hyperglycemia Ratio, and Functional Outcomes in Patients With Acute Ischemic Stroke Treated With Intravenous Thrombolysis
Abstract
Background: Stress hyperglycemia ratio (SHR), calculated as glucose/glycated hemoglobin, has recently been developed for assessing stress hyperglycemia and could provide prognostic information for various diseases. However, calculating SHR using random blood glucose (RBG) drawn on admission or fasting blood glucose (FBG) could lead to different results. This study intends to evaluate the association between SHR and functional outcomes in patients with acute ischemic stroke (AIS) with recombinant tissue plasminogen activator (r-tPA) intravenous thrombolysis.
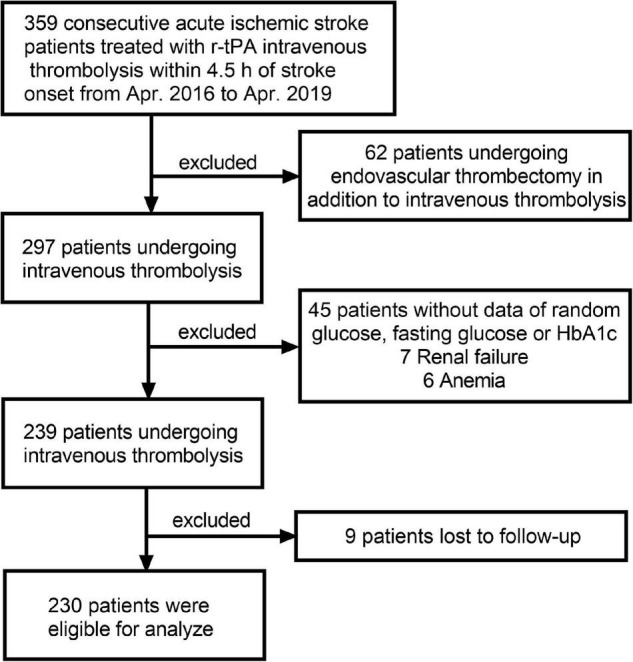
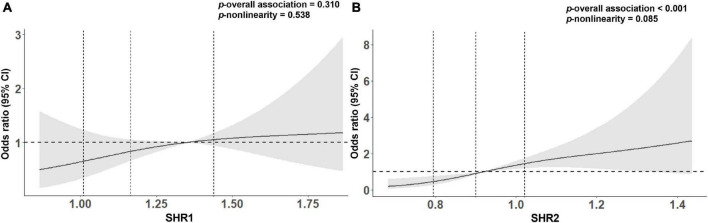
Methods: Data from 230 patients with AIS following thrombolytic therapy with r-tPA in the Third Affiliated Hospital of Wenzhou Medical University from April 2016 to April 2019 were retrospectively reviewed. SHR1 was defined as [RBG (mmol/L)]/[HbA1c (%)] and SHR2 was defined as [FBG (mmol/L)]/[HbA1c (%)]. The outcomes included early neurological improvement (ENI), poor function defined as a modified Rankin Scale score (mRS) of 3-6, and all-cause death in 3 months. Multivariable logistic regression was performed to estimate the association between SHR and adverse outcomes.
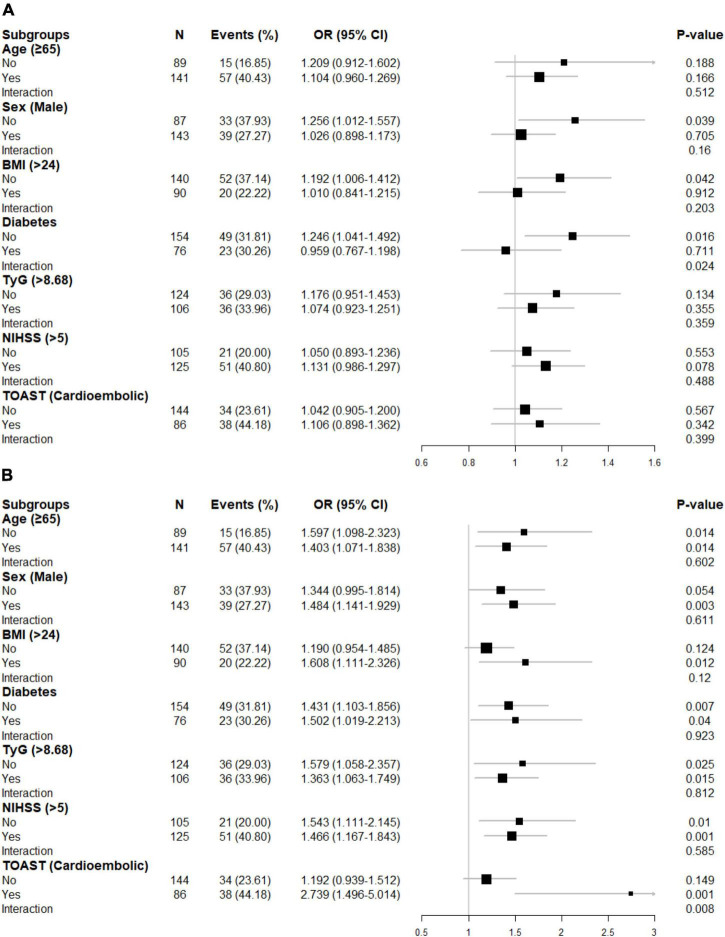
Results: After adjustment for possible confounders, though patients with AIS with higher SHR1 tend to have a higher risk of poor outcome and death and unlikely to develop ENI, these did not reach the statistical significance. In contrast, SHR2 was independently associated with poor functional outcome (per 0.1-point increases: odds ratios (OR) = 1.383 95% CI [1.147-1.668]). Further adjusted for body mass index (BMI), triglyceride-glucose index (TyG), and diabetes slightly strengthen the association between SHR (both 1 and 2) and adverse outcomes. In subgroup analysis, elevated SHR1 is associated with poor functional outcomes (per 0.1-point increases: OR = 1.246 95% CI [1.041-1.492]) in non-diabetic individuals and the association between SHR2 and the poor outcomes was attenuated in non-cardioembolic AIS.
Conclusion: SHR is expected to replace random or fasting glucose concentration as a novel generation of prognostic indicator and a potential therapeutic target.
Keywords: fasting blood glucose; intravenous thrombolysis; random blood glucose; stress hyperglycemia ratio; stroke.
Copyright © 2022 Chen, Ren, Huang, Shen, Yang, Hu, Pan, Sun, Zhou, Zeng, Li, Yang and Weng.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Adams H. P., Bendixen B. H., Kappelle L. J., Biller J., Love B. B., Gordon D. L., et al. (1993). Classification of subtype of acute ischemic stroke. Definitions for use in a multicenter clinical trial. TOAST. Trial of Org 10172 in Acute Stroke Treatment. Stroke 24 35–41. 10.1161/01.Str.24.1.35 - DOI - PubMed
-
- Dietrich W. D., Alonso O., Busto R. (1993). Moderate hyperglycemia worsens acute blood-brain barrier injury after forebrain ischemia in rats. Stroke 24 111–116. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous