

RICORS2040: the need for collaborative research in chronic kidney disease
- PMID: 35211298
- PMCID: PMC8862113
- DOI: 10.1093/ckj/sfab170
RICORS2040: the need for collaborative research in chronic kidney disease
Abstract
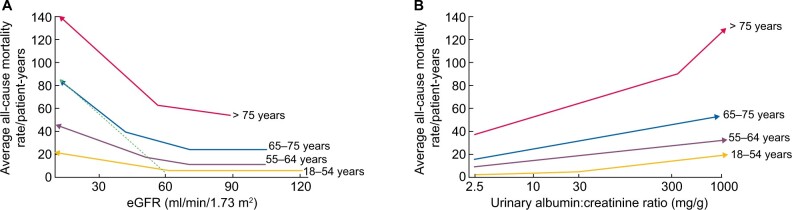
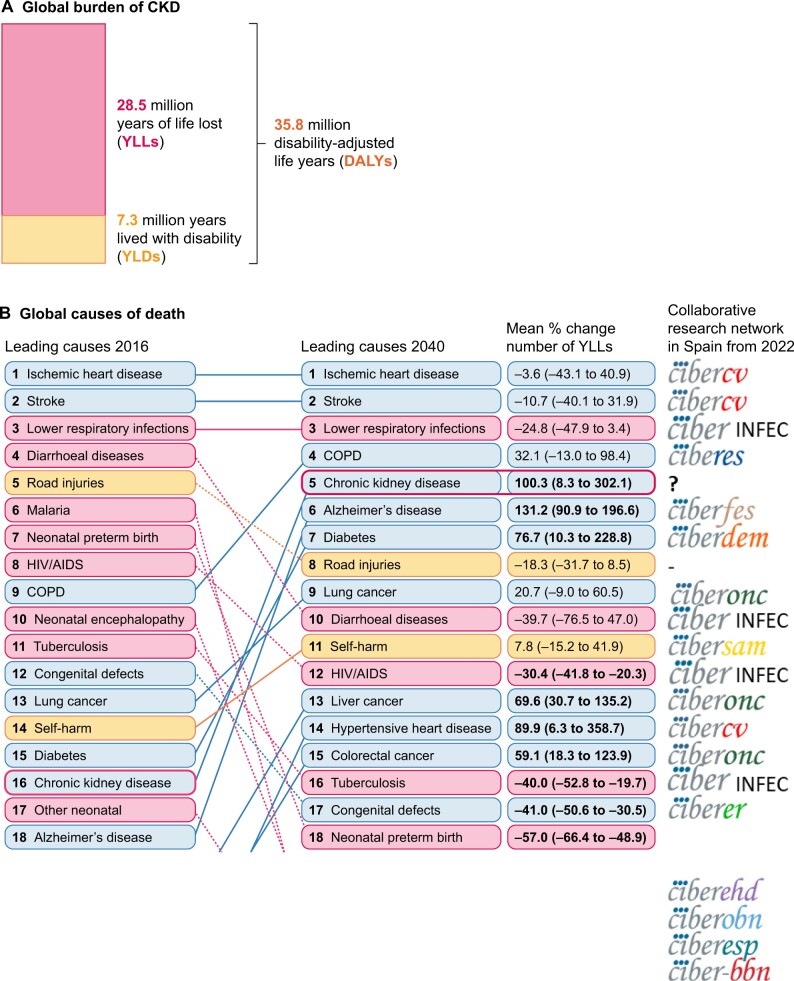
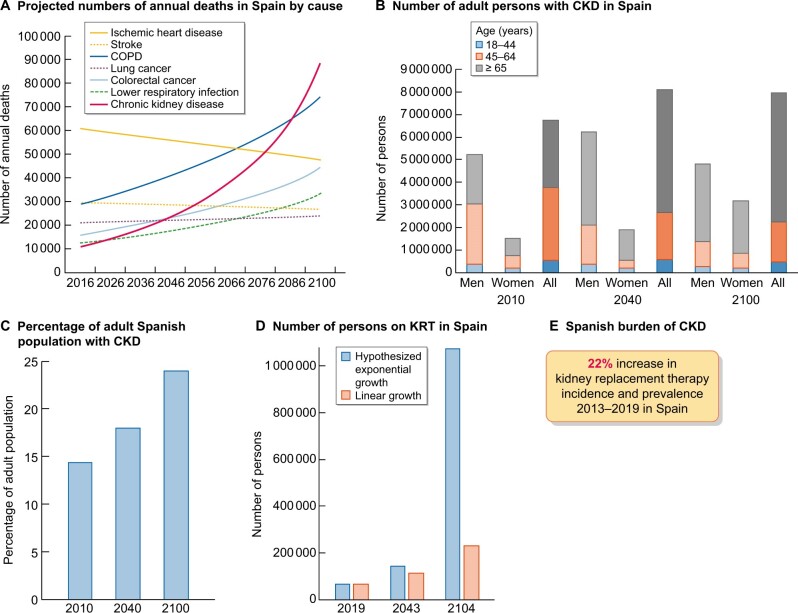
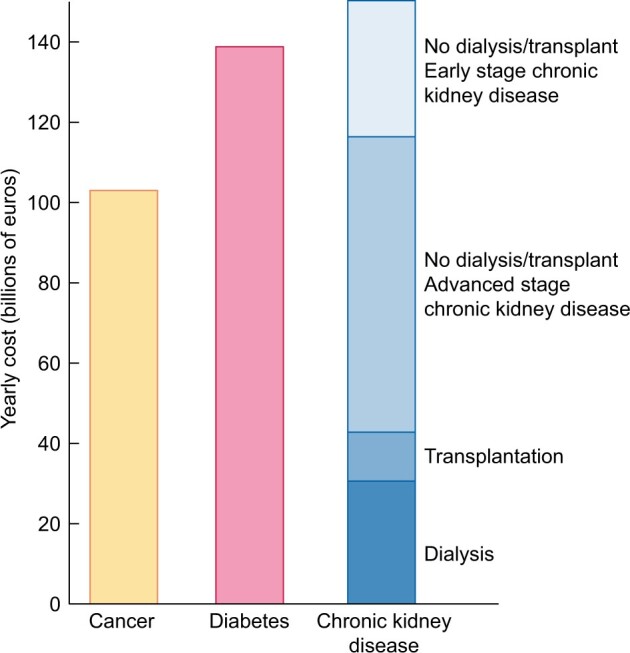
Chronic kidney disease (CKD) is a silent and poorly known killer. The current concept of CKD is relatively young and uptake by the public, physicians and health authorities is not widespread. Physicians still confuse CKD with chronic kidney insufficiency or failure. For the wider public and health authorities, CKD evokes kidney replacement therapy (KRT). In Spain, the prevalence of KRT is 0.13%. Thus health authorities may consider CKD a non-issue: very few persons eventually need KRT and, for those in whom kidneys fail, the problem is 'solved' by dialysis or kidney transplantation. However, KRT is the tip of the iceberg in the burden of CKD. The main burden of CKD is accelerated ageing and premature death. The cut-off points for kidney function and kidney damage indexes that define CKD also mark an increased risk for all-cause premature death. CKD is the most prevalent risk factor for lethal coronavirus disease 2019 (COVID-19) and the factor that most increases the risk of death in COVID-19, after old age. Men and women undergoing KRT still have an annual mortality that is 10- to 100-fold higher than similar-age peers, and life expectancy is shortened by ~40 years for young persons on dialysis and by 15 years for young persons with a functioning kidney graft. CKD is expected to become the fifth greatest global cause of death by 2040 and the second greatest cause of death in Spain before the end of the century, a time when one in four Spaniards will have CKD. However, by 2022, CKD will become the only top-15 global predicted cause of death that is not supported by a dedicated well-funded Centres for Biomedical Research (CIBER) network structure in Spain. Realizing the underestimation of the CKD burden of disease by health authorities, the Decade of the Kidney initiative for 2020-2030 was launched by the American Association of Kidney Patients and the European Kidney Health Alliance. Leading Spanish kidney researchers grouped in the kidney collaborative research network Red de Investigación Renal have now applied for the Redes de Investigación Cooperativa Orientadas a Resultados en Salud (RICORS) call for collaborative research in Spain with the support of the Spanish Society of Nephrology, Federación Nacional de Asociaciones para la Lucha Contra las Enfermedades del Riñón and ONT: RICORS2040 aims to prevent the dire predictions for the global 2040 burden of CKD from becoming true.
Keywords: COVID-19; accelerated ageing; burden of disease; chronic kidney disease; decade of the kidney; kidney failure; kidney transplantation; research funding.
© The Author(s) 2021. Published by Oxford University Press on behalf of the ERA.
Figures


Comment in
-
Use of nephrotoxic medications in adults with chronic kidney disease in Swedish and US routine care.Clin Kidney J. 2021 Oct 29;15(3):442-451. doi: 10.1093/ckj/sfab210. eCollection 2022 Mar. Clin Kidney J. 2021. PMID: 35296039 Free PMC article.
Comment on
-
More on the invisibility of chronic kidney disease… and counting.Clin Kidney J. 2021 Nov 27;15(3):388-392. doi: 10.1093/ckj/sfab240. eCollection 2022 Mar. Clin Kidney J. 2021. PMID: 35198154 Free PMC article.
References
-
- Kidney Disease: Improving Global Outcomes CKD Work Group. KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int Suppl 2013; 3: 1–150 - PubMed
-
- Ortiz A, Covic A, Fliser D. et al. Epidemiology, contributors to, and clinical trials of mortality risk in chronic kidney failure. Lancet 2014; 383: 1831–1843 - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
