

Urine metabolic risk factors and outcomes of patients with kidney transplant nephrolithiasis
- PMID: 35211306
- PMCID: PMC8862062
- DOI: 10.1093/ckj/sfab208
Urine metabolic risk factors and outcomes of patients with kidney transplant nephrolithiasis
Abstract
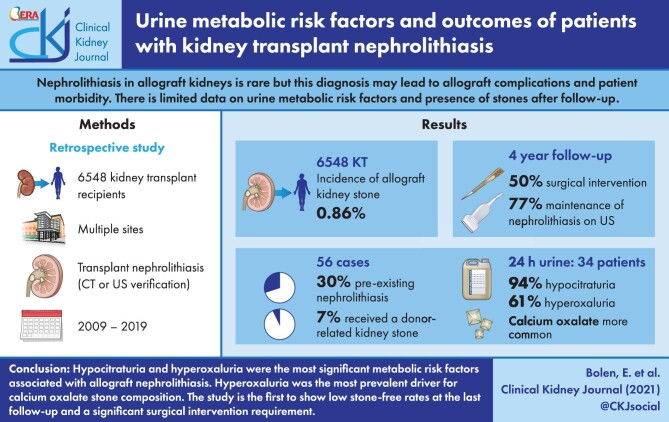
Background: Nephrolithiasis in allograft kidneys is rare, but this diagnosis may lead to allograft complications and patient morbidity. Previous studies that have evaluated nephrolithiasis posttransplant have focused on surgical stone management, with limited data on urine metabolic risk factors and the presence of stones after follow-up.
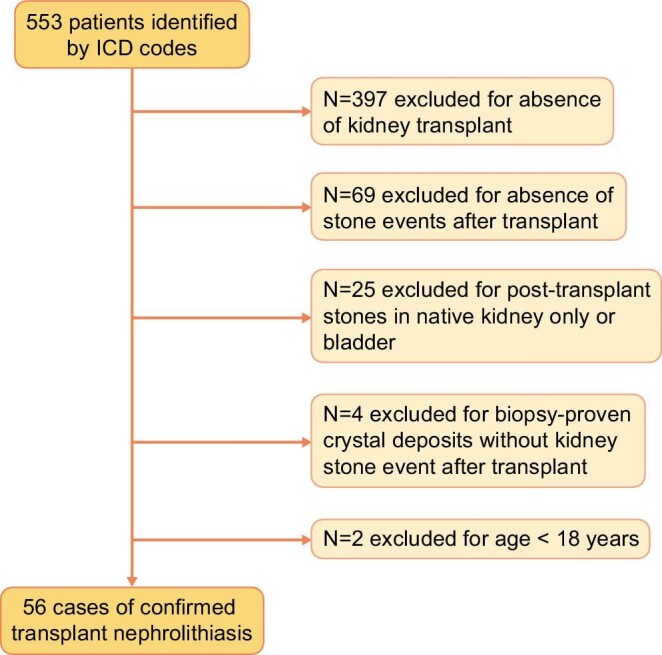
Methods: We retrospectively evaluated kidney transplant recipients who were diagnosed with transplant nephrolithiasis between 2009 and 2019. Computed tomography and ultrasound imaging were used to confirm stone presence.
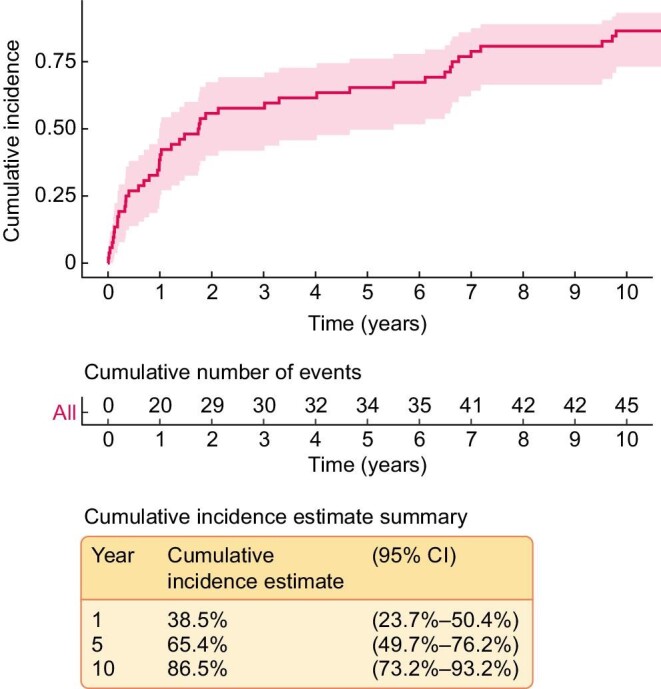
Results: The incidence of allograft kidney stone formation was 0.86% of 6548 kidney transplant recipients. Of the 56 cases identified, 17 (30%) had a pretransplant history of nephrolithiasis. Only four (7%) patients received a known kidney stone at the time of allograft implantation. Of the 56 cases, 34 had a 24-h supersaturation study. The urine supersaturation study showed 32 patients (94%) had a urine citrate of <450 mg excreted in 24 h (median 124.5 mg/24 h, reference range >500 mg/24 h), along with 22 patients (61%) having a urine oxalate excretion of ≥30 mg in 24 h (median 34.4 mg/24 h, reference range <30 mg/24 h). Calcium oxalate composition was most common (91% with >1 supersaturation for calcium oxalate crystals), with normal median urine calcium levels (median urine calcium 103.5 mg/24 h, reference range <200 mg/24 h). After a 4-year follow-up, 50% (n = 28) required surgical intervention and 43 (77%) patients continued to have evidence of transplant nephrolithiasis on imaging.
Conclusions: This is the largest study of transplant nephrolithiasis confirming that hypocitraturia and hyperoxaluria were the most significant urine metabolic risk factors associated with allograft nephrolithiasis and that hyperoxaluria was the most prevalent driver for calcium oxalate stone composition. Our study is first to show low stone-free rates at the last follow-up and a significant proportion requiring surgical intervention.
Keywords: hyperoxaluria; hypocitraturia; kidney stone; kidney transplantation; nephrolithiasis.
© The Author(s) 2021. Published by Oxford University Press on behalf of the ERA.
Figures
References
-
- Stravodimos KG, Adamis S, Tyritzis Set al. Renal transplant lithiasis: analysis of our series and review of the literature. J Endourol 2012; 26: 38–44 - PubMed
-
- Ferreira Cassini M, Cologna AJ, Ferreira Andrade Met al. Lithiasis in 1,313 kidney transplants: incidence, diagnosis, and management. Transplant Proc 2012; 44: 2373–2375 - PubMed
LinkOut - more resources
Full Text Sources
