

Clinical Landscape of Littoral Cell Angioma in the Spleen Based on a Comprehensive Analysis
- PMID: 35211400
- PMCID: PMC8861295
- DOI: 10.3389/fonc.2022.790332
Clinical Landscape of Littoral Cell Angioma in the Spleen Based on a Comprehensive Analysis
Abstract
Objective: Littoral cell angioma (LCA) is currently considered to be a rare splenic tumor with malignant potential. As the epidemiology, pathogenesis, clinical manifestation, treatment, and prognosis remain unclear, the clinical diagnosis and treatment of LCA have not been standardized. Hence, we performed a comprehensive analysis of 189 observational studies comprising 435 patients to improve the current status of diagnosis and treatment.
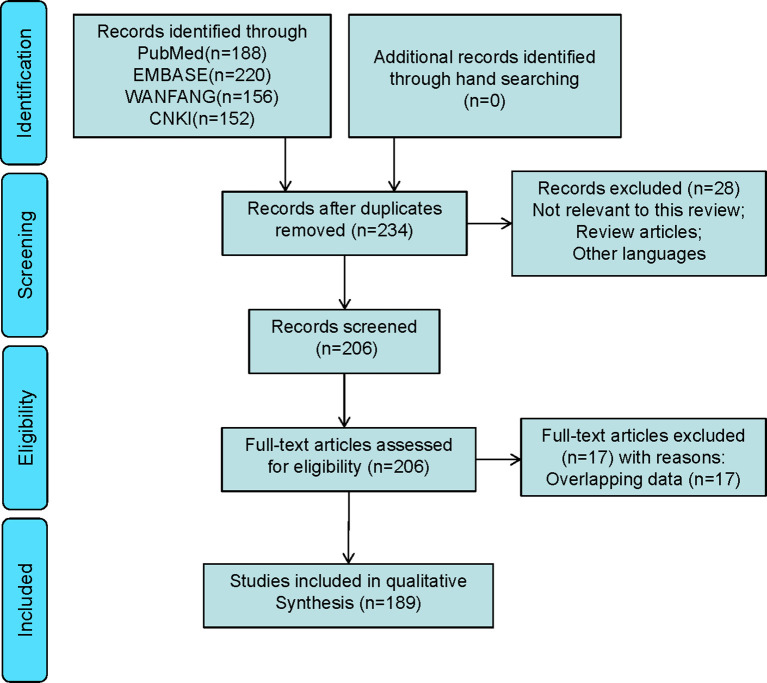
Methods: PubMed, Embase, WanFang and CNKI were searched from inception to May 2021 to identify LCA studies that were published in English and Chinese. The clinical information of LCA patients were extracted and analyzed.
Results: The LCA has a male-to-female ratio of 0.90 and a solitary-to-multiple ratio of 0.31. In terms of clinical features, 69.7% of the patients showed splenomegaly, 49.7% were asymptomatic, and 39.2% experienced epigastric discomfort. As the imaging findings of patients with LCA were nonspecific, an image-guided biopsy (10/12) was a safe and effective method for diagnosing in this condition. Notably, results of the prognostic analysis indicated that LCA has a lower risk of recurrence and metastasis. The patient may develop a stable disease or the tumor will grow but will not metastasize. Besides, the novel immunohistochemical pattern of LCA was described as CD31+/ERG+/FVIII Antigen+/CD68+/CD163+/lysozyme+/CD8-/WT1-.
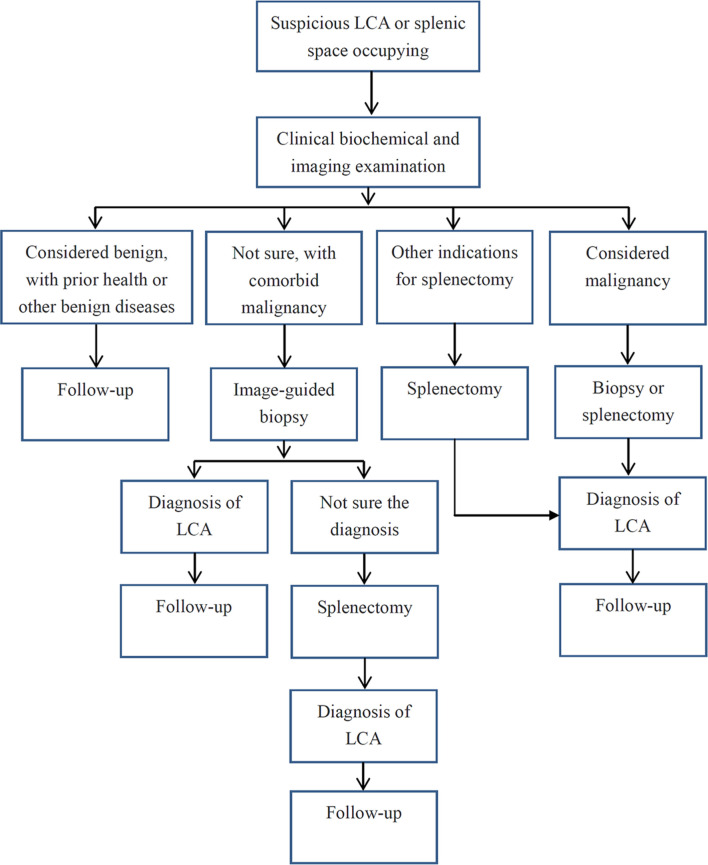
Conclusion: LCA should be reconsidered as a benign primary splenic vascular neoplasm, which is more like an intra-splenic manifestation of abnormal body function. Image-guided biopsy with follow-up might be a beneficial choice for LCA patients. For LCA patients with abdominal discomfort, pathological uncertainty or continuous tumor enlargement, splenectomy remains the preferred treatment.
Keywords: diagnosis; littoral cell angioma; prognosis; systematic review; treatment.
Copyright © 2022 Wang, Qi, Zhao, Zhang, Zhu, Liang and Sun.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures



Similar articles
-
Case report and literature review: Asymptomatic littoral cell angioma in a 3-year-old girl.Front Pediatr. 2024 Apr 18;12:1383015. doi: 10.3389/fped.2024.1383015. eCollection 2024. Front Pediatr. 2024. PMID: 38699151 Free PMC article.
-
Atypical immunophenotype in a littoral cell angioma.Vojnosanit Pregl. 2009 Jan;66(1):63-5. doi: 10.2298/vsp0901063c. Vojnosanit Pregl. 2009. PMID: 19195267
-
Case report: Infrequent littoral cell angioma of the spleen.Int J Surg Case Rep. 2021 Aug;85:106242. doi: 10.1016/j.ijscr.2021.106242. Epub 2021 Jul 27. Int J Surg Case Rep. 2021. PMID: 34333257 Free PMC article.
-
The splenic Littoral cell angioma in China: a case report and review.World J Surg Oncol. 2011 Dec 15;9:168. doi: 10.1186/1477-7819-9-168. World J Surg Oncol. 2011. PMID: 22172167 Free PMC article. Review.
-
Littoral cell angioma of the spleen: A study of 10 cases case series and literature review.Medicine (Baltimore). 2024 Mar 29;103(13):e37550. doi: 10.1097/MD.0000000000037550. Medicine (Baltimore). 2024. PMID: 38552075 Free PMC article. Review.
Cited by
-
Littoral Cell Angioma of the Spleen: A Case Report.Cureus. 2023 Apr 4;15(4):e37137. doi: 10.7759/cureus.37137. eCollection 2023 Apr. Cureus. 2023. PMID: 37153304 Free PMC article.
-
Case report and literature review: Asymptomatic littoral cell angioma in a 3-year-old girl.Front Pediatr. 2024 Apr 18;12:1383015. doi: 10.3389/fped.2024.1383015. eCollection 2024. Front Pediatr. 2024. PMID: 38699151 Free PMC article.
-
Application of Nuclear Medicine Liver-Spleen Scan for Evaluation of Littoral Cell Angioma of the Spleen: A Case Report.J Investig Med High Impact Case Rep. 2025 Jan-Dec;13:23247096251350571. doi: 10.1177/23247096251350571. Epub 2025 Jun 25. J Investig Med High Impact Case Rep. 2025. PMID: 40556473 Free PMC article.
-
The first case of a littoral spleen-preserving resection: a case report.J Surg Case Rep. 2023 Oct 20;2023(10):rjad563. doi: 10.1093/jscr/rjad563. eCollection 2023 Oct. J Surg Case Rep. 2023. PMID: 37867921 Free PMC article.
-
The Spectrum of Solitary Benign Splenic Lesions-Imaging Clues for a Noninvasive Diagnosis.Diagnostics (Basel). 2023 Jun 20;13(12):2120. doi: 10.3390/diagnostics13122120. Diagnostics (Basel). 2023. PMID: 37371015 Free PMC article. Review.
References
Publication types
LinkOut - more resources
Full Text Sources
Research Materials