

Comparison of the clinical performance of i-gel and Ambu laryngeal masks in anaesthetised paediatric patients: A meta-analysis
- PMID: 35211557
- PMCID: PMC8855187
- DOI: 10.12998/wjcc.v10.i4.1242
Comparison of the clinical performance of i-gel and Ambu laryngeal masks in anaesthetised paediatric patients: A meta-analysis
Abstract
Background: Paediatric supraglottic airway devices (SGAs) are widely used in routine anaesthesia and serve as primary or back-up devices for difficult airway management. The inflatable Ambu laryngeal masks and non-inflatable i-gel are two improvements of SGAs based on classic laryngeal masks. The clinical performance and safety of these two devices in paediatric patients are still unclear and warrant further investigation.
Aim: To perform a systematic review and meta-analysis on the clinical performance and safety of Ambu laryngeal masks and i-gel in anaesthetised paediatric patients.
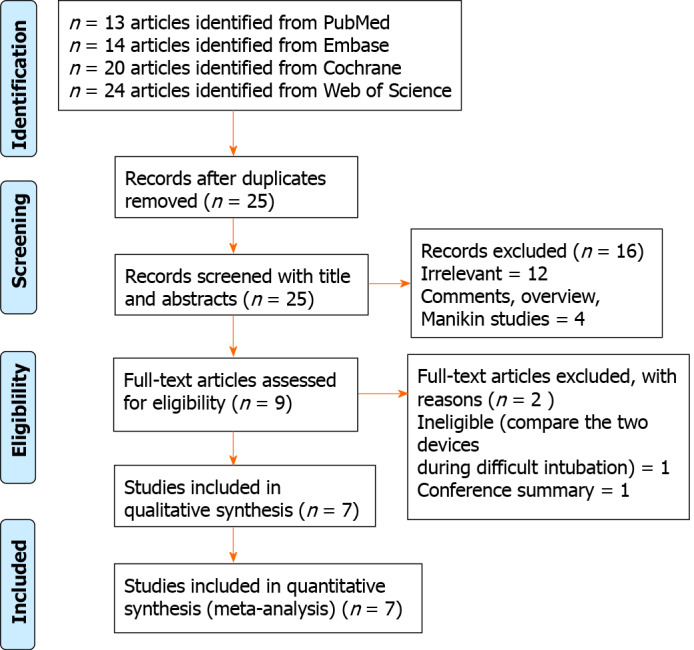
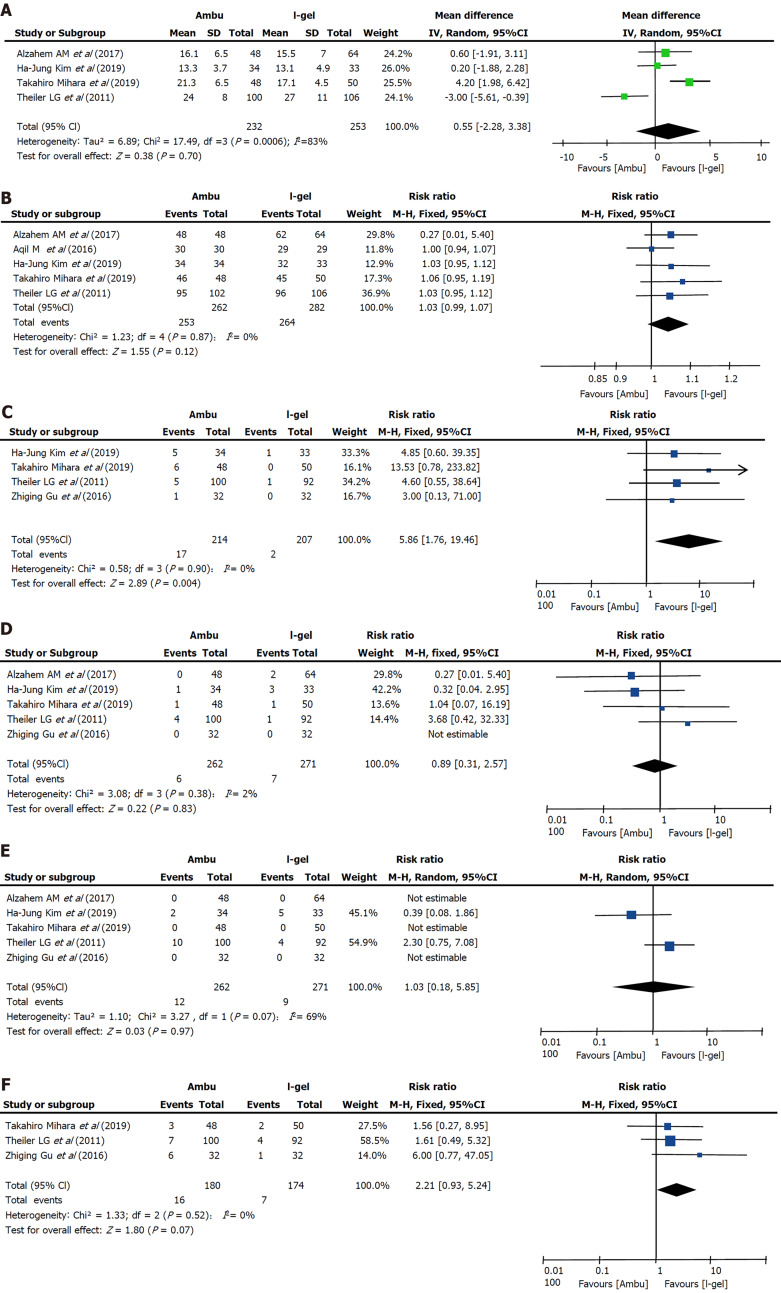
Methods: MEDLINE, Embase, Web of Science and Cochrane Central Register of Controlled Trials were searched from inception dates to April 2020. We identified published randomised controlled trials (RCTs) in which the intervention involved the use of Ambu laryngeal masks and i-gel in anaesthetised paediatric patients (age < 18 years). We assessed the oropharyngeal leak pressure (OLP) as the primary outcome. The secondary outcomes were insertion time, success rate of insertion on the first attempt, and incidence of adverse events.
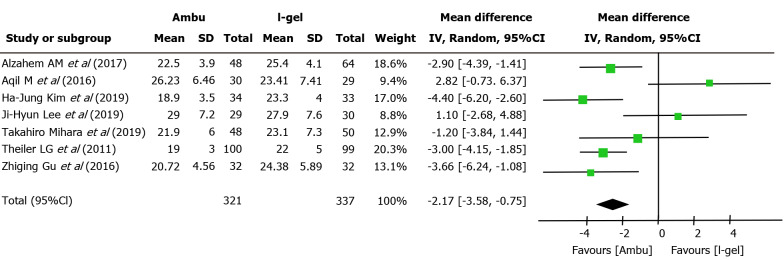
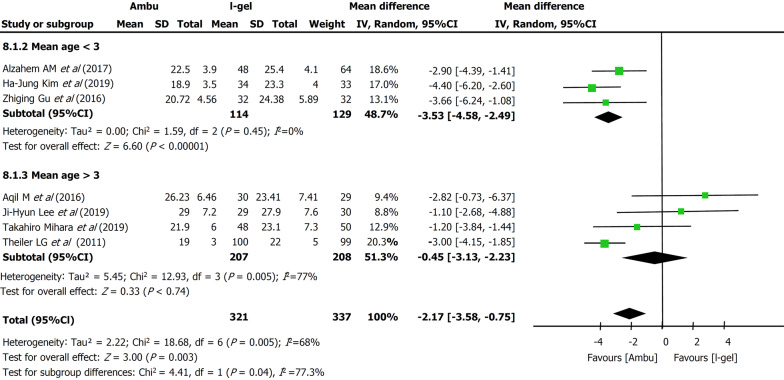
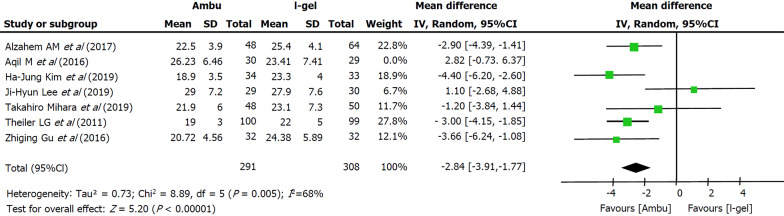
Results: After searching for all relevant trials published up to April 2020, data from seven RCTs with a total of 667 paediatric patients (323 and 344 participants in the i-gel and Ambu groups, respectively) were evaluated. The mean OLP in anaesthetised paediatric patients was lower in the Ambu group [21.82 cmH2O for Ambu vs 23.98 cmH2O for i-gel, P = 0.003, 95% confidence interval (CI): -3.58 to -0.75, I 2 = 68%, Mantel-Haenszel random model]. We did not find any clear evidence of differences between the devices in terms of insertion time, success rate of insertion, and incidence of adverse events except for blood staining (risk ratio 5.86, 95%CI: 1.76 to 19.46, P = 0.004, I 2 = 0, fixed-effect model).
Conclusion: The i-gel airway may provide a better seal and is therefore probably more suitable than the Ambu laryngeal mask airway in anaesthetised paediatric patients. However, the evidence is insufficient to allow making firm conclusions or to guide clinical practice, owing to the small number of relevant published studies.
Keywords: Ambu laryngeal masks; Clinical performance; I-gel; Pediatric.
©The Author(s) 2022. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: The authors declare that they have no competing interests.
Figures
Similar articles
-
Comparison of Ambu AuraGain and BlockBuster laryngeal mask for controlled ventilation in children undergoing minor surgical procedures under general anesthesia: A prospective randomized controlled study.Paediatr Anaesth. 2023 Jun;33(6):474-480. doi: 10.1111/pan.14653. Epub 2023 Mar 16. Paediatr Anaesth. 2023. PMID: 36866955 Clinical Trial.
-
Comparison of the clinical performance of i-gel and Ambu AuraGain in children: A randomised noninferiority clinical trial.Eur J Anaesthesiol. 2019 Jun;36(6):411-417. doi: 10.1097/EJA.0000000000000987. Eur J Anaesthesiol. 2019. PMID: 30950904 Clinical Trial.
-
Randomised crossover comparison of the Ambu AuraOnce Laryngeal Mask with the LMA Classic laryngeal mask airway in paralysed anaesthetised patients.Anaesthesia. 2008 Jan;63(1):82-5. doi: 10.1111/j.1365-2044.2007.05284.x. Anaesthesia. 2008. PMID: 18086075 Clinical Trial.
-
Evaluation of i-gel(™) airway in children: a meta-analysis.Paediatr Anaesth. 2014 Oct;24(10):1072-9. doi: 10.1111/pan.12483. Epub 2014 Jul 16. Paediatr Anaesth. 2014. PMID: 25041224 Review.
-
Laryngeal mask airway ProSeal provides higher oropharyngeal leak pressure than i-gel in adult patients under general anesthesia: a meta-analysis.J Clin Anesth. 2016 Sep;33:298-305. doi: 10.1016/j.jclinane.2016.04.020. Epub 2016 May 18. J Clin Anesth. 2016. PMID: 27555181 Review.
Cited by
-
Anesthesia management for a child with the Koolen-de Vries syndrome: a case report.BMC Anesthesiol. 2024 Apr 13;24(1):143. doi: 10.1186/s12871-024-02508-7. BMC Anesthesiol. 2024. PMID: 38614993 Free PMC article.
-
Ventilation practices and preparedness of healthcare providers in term newborn resuscitation: A comprehensive survey study in Austrian hospitals.Resusc Plus. 2024 Nov 7;20:100817. doi: 10.1016/j.resplu.2024.100817. eCollection 2024 Dec. Resusc Plus. 2024. PMID: 39559729 Free PMC article.
References
-
- White MC, Cook TM, Stoddart PA. A critique of elective pediatric supraglottic airway devices. Paediatr Anaesth. 2009;19 Suppl 1:55–65. - PubMed
-
- Goel D, Shah D, Hinder M, Tracy M. Laryngeal mask airway use during neonatal resuscitation: a survey of practice across newborn intensive care units and neonatal retrieval services in Australian New Zealand Neonatal Network. J Paediatr Child Health. 2020;56:1346–1350. - PubMed
-
- Luce V, Harkouk H, Brasher C, Michelet D, Hilly J, Maesani M, Diallo T, Mangalsuren N, Nivoche Y, Dahmani S. Supraglottic airway devices vs tracheal intubation in children: a quantitative meta-analysis of respiratory complications. Paediatr Anaesth. 2014;24:1088–1098. - PubMed
-
- Keller C, Brimacombe J, Bittersohl J, Lirk P, von Goedecke A. Aspiration and the laryngeal mask airway: three cases and a review of the literature. Br J Anaesth. 2004;93:579–582. - PubMed
-
- Griffin RM, Hatcher IS. Aspiration pneumonia and the laryngeal mask airway. Anaesthesia. 1990;45:1039–1040. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
