

Aseptic abscess in the abdominal wall accompanied by monoclonal gammopathy simulating the local recurrence of rectal cancer: A case report
- PMID: 35211612
- PMCID: PMC8855253
- DOI: 10.12998/wjcc.v10.i5.1702
Aseptic abscess in the abdominal wall accompanied by monoclonal gammopathy simulating the local recurrence of rectal cancer: A case report
Abstract
Background: Infectious abscesses in the abdominal wall can be secondary to retained foreign bodies (e.g., stones, use of artificial mesh, use of silk yarn in surgical suture), inflammatory diseases (e.g., acute appendicitis), and perforated malignancies of the digestive tract (particularly the colon). Aseptic abscesses (AAs) are relatively rare. To the best of our knowledge, this is the first report of an AA in the abdominal wall accompanied by monoclonal gammopathy of undetermined significance (MGUS) at 5 years after laparoscopic proctectomy.
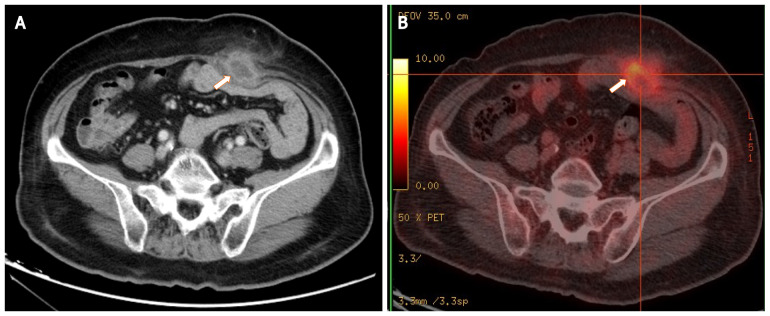
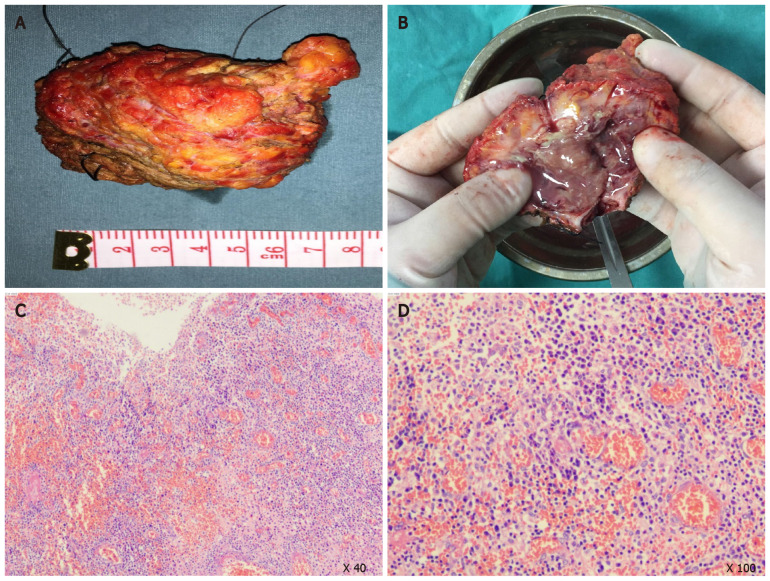
Case summary: A 72-year-old female patient presented with an enlarged painless mass in the lower abdomen for 1 year. She had a history of obesity, diabetes, and MGUS. Her surgical history was laparoscopic resection for rectal cancer 6 years prior, followed by chemotherapy. She was afebrile. Abdominal examination revealed a smooth abdomen with a clinically palpable solid mass under a laparotomy scar in the left lower quadrant. No obvious tenderness or skin redness was spotted. Laboratory data were not remarkable. Computed tomography scan revealed a low-density mass of 4.8 cm in diameter in the lower abdominal wall, which showed high uptake on positron emission tomography. The preoperative diagnosis was an abscess or tumor, and surgical resection was recommended. The mass was confirmed to be an AA by microbiological and pathological examinations. The patient recovered well after surgery. There was no evidence of recurrence 2 years later.
Conclusion: It is important to consider underlying conditions (diabetes, chemotherapy, MGUS) which may contribute to AA formation in the surgical wound.
Keywords: Abdominal wall; Aseptic abscess; Case report; Laparoscopic resection; Monoclonalgammopathy of undetermined significance; Rectal cancer.
©The Author(s) 2022. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: The authors declare that they have no conflicts of interest.
Figures
Similar articles
-
Delayed abdominal wall abscess after abdomino-perineal resection simulating local recurrence of rectal cancer.Springerplus. 2014 Nov 20;3:681. doi: 10.1186/2193-1801-3-681. eCollection 2014. Springerplus. 2014. PMID: 25520908 Free PMC article.
-
Diffuse Peritoneal and Bowel Wall Infiltration by Light Chain-AL Amyloidosis with Omental Calcification Mimicking Abdominal Carcinomatosis - An Elderly Female with Incidental Finding of Light Chain Monoclonal Gammopathy of Undetermined Significance (LC-MGUS).Am J Case Rep. 2017 Nov 25;18:1247-1250. doi: 10.12659/ajcr.907041. Am J Case Rep. 2017. PMID: 29176541 Free PMC article.
-
Management of refractory metastatic anal squamous cell carcinoma following disease progression on traditional chemoradiation therapy.J Adv Pract Oncol. 2012 May;3(3):161-9. doi: 10.6004/jadpro.2012.3.3.4. J Adv Pract Oncol. 2012. PMID: 25031942 Free PMC article.
-
Aseptic abscesses: a study of 30 patients with or without inflammatory bowel disease and review of the literature.Medicine (Baltimore). 2007 May;86(3):145-161. doi: 10.1097/md.0b013e18064f9f3. Medicine (Baltimore). 2007. PMID: 17505254 Review.
-
[Diffuse plane normolipemic xanthomatosis and necrobiotic xanthogranuloma associated with monoclonal gammopathy--determining the disease stage with PET-CT and treatment experience. Two case studies and literature review].Vnitr Lek. 2010 Nov;56(11):1158-68. Vnitr Lek. 2010. PMID: 21250495 Review. Czech.
Cited by
-
Aseptic Abscess of the Gallbladder Mimicking Gallbladder Carcinoma after Surgery for Ulcerative Colitis.Intern Med. 2025 Jul 1;64(13):1984-1992. doi: 10.2169/internalmedicine.4411-24. Epub 2024 Dec 5. Intern Med. 2025. PMID: 39631865 Free PMC article.
References
-
- Amer E, Er A, Cengiz F, Karaisli S, Peskersoy M. Colon Cancer Presenting as Abdominal Wall Abscess. Cyprus J Med Sci. 2018;3:202–203.
-
- Snast I, Ostfeld I, Pavlovsky L, Hodak E, Gafter-Gvili A. Pyoderma Gangrenosum and Extensive Aseptic Chest Wall Abscess in a Patient with Inflammatory Bowel Disease. Isr Med Assoc J. 2018;20:712–713. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
