

The state of diabetes treatment coverage in 55 low-income and middle-income countries: a cross-sectional study of nationally representative, individual-level data in 680 102 adults
- PMID: 35211689
- PMCID: PMC8865379
- DOI: 10.1016/s2666-7568(21)00089-1
The state of diabetes treatment coverage in 55 low-income and middle-income countries: a cross-sectional study of nationally representative, individual-level data in 680 102 adults
Abstract
Background: Approximately 80% of the 463 million adults worldwide with diabetes live in low- and middle-income countries (LMICs). A major obstacle to designing evidence-based policies to improve diabetes outcomes in LMICs is the limited nationally representative data on the current patterns of treatment coverage. The objectives of this study are (1) to estimate the proportion of adults with diabetes in LMICs who receive coverage of recommended pharmacological and non-pharmacological diabetes treatment and (2) to describe country-level and individual-level characteristics that are associated with treatment.
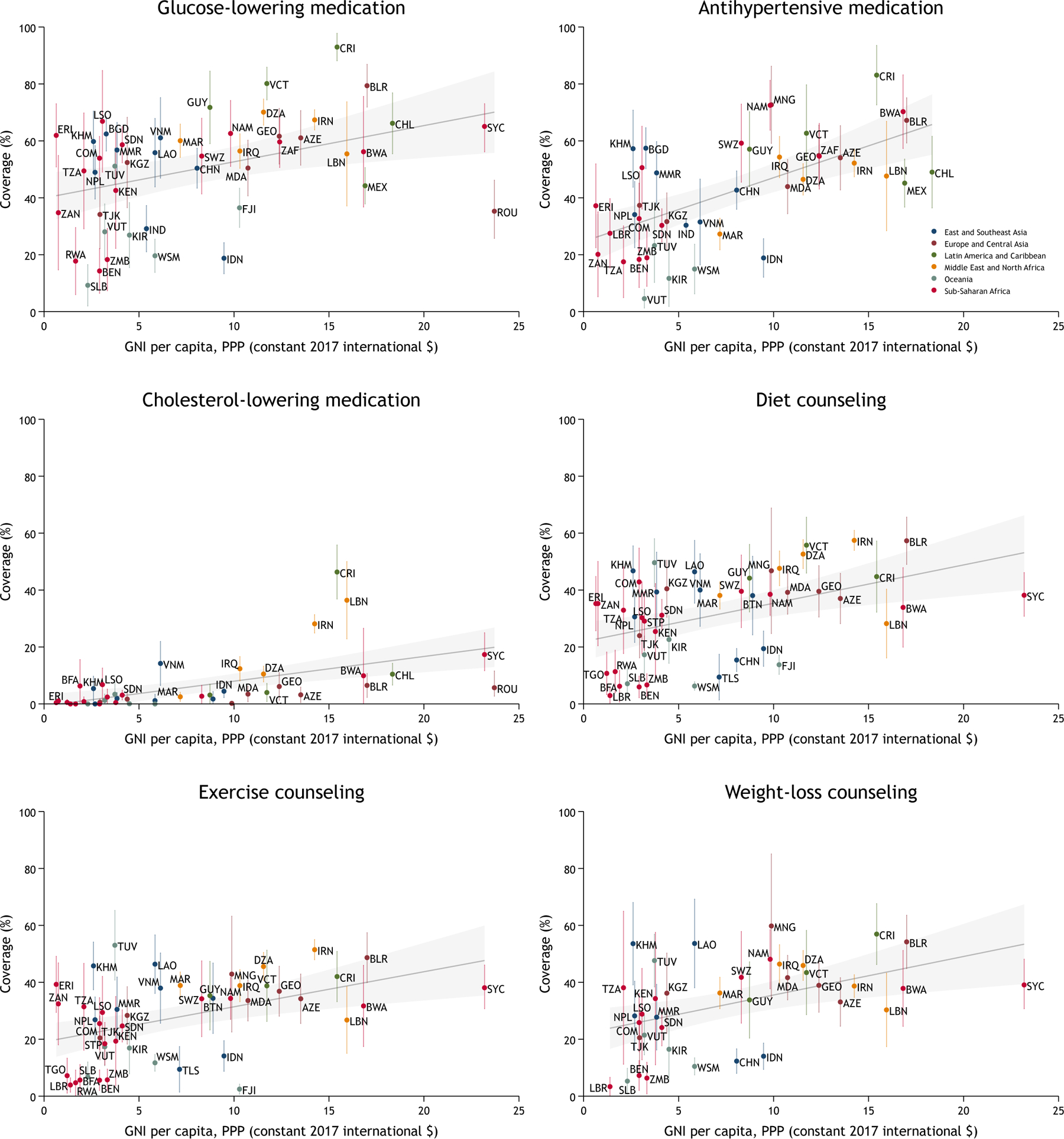
Methods: We conducted a cross-sectional analysis of pooled, individual data from 55 nationally representative surveys in LMICs. Our primary outcome of self-reported diabetes treatment coverage was based upon population-level monitoring indicators recommended in the 2020 World Health Organization Package of Essential Noncommunicable Disease Interventions. We assessed coverage of three pharmacological and three non-pharmacological treatments among people with diabetes. At the country level, we estimated the proportion of individuals reporting coverage by per-capita gross national income and geographic region. At the individual level, we used logistic regression models to assess coverage along several key individual characteristics including sex, age, BMI, wealth quintile, and educational attainment. In the primary analysis, we scaled sample weights such that countries were weighted equally.
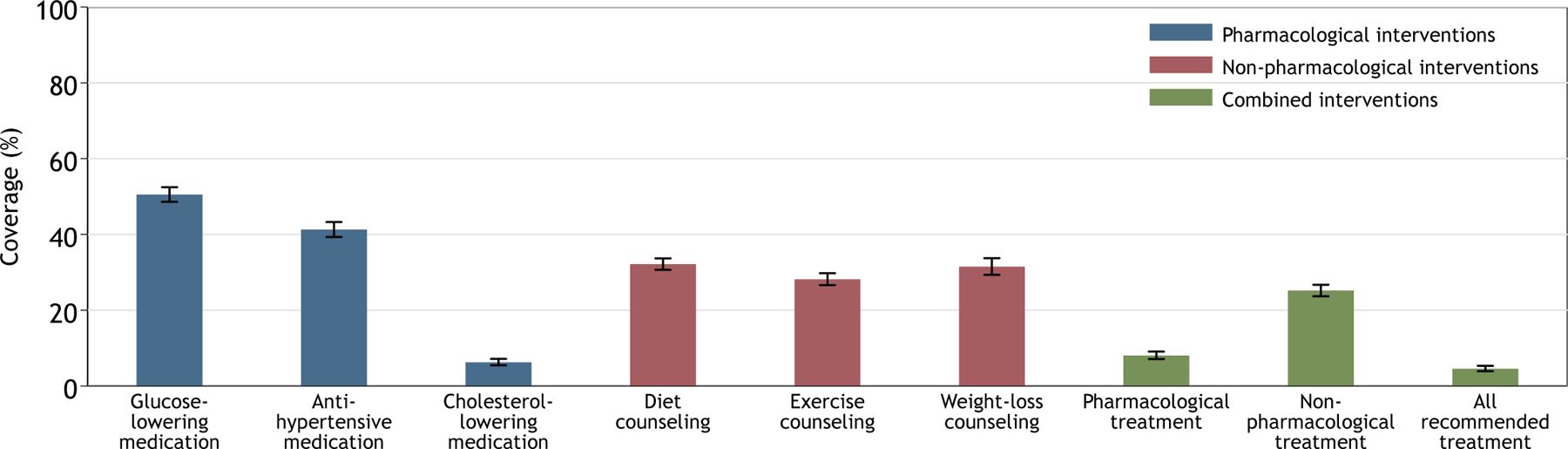
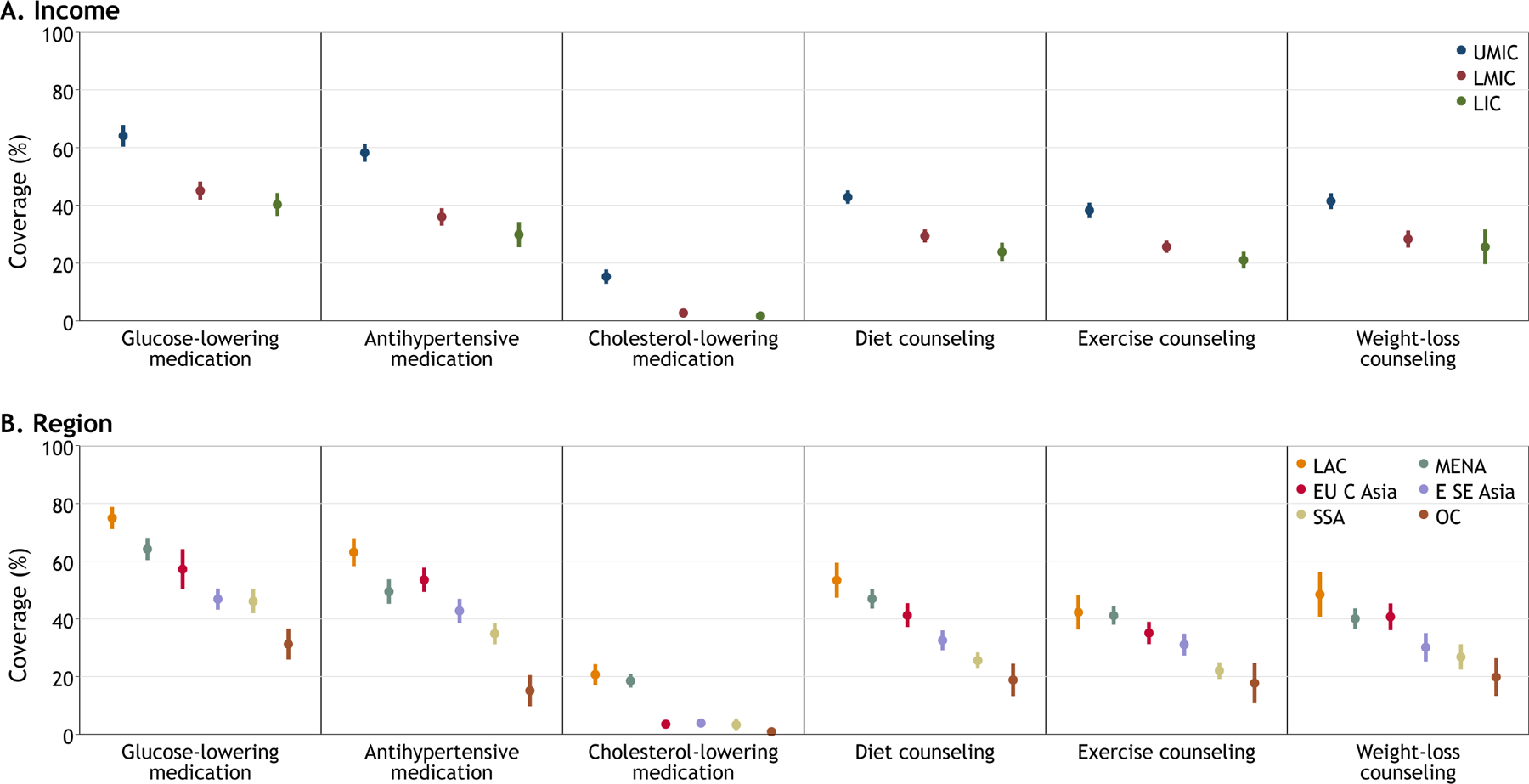
Findings: The final pooled sample from the 55 LMICs included 680,102 total individuals and 37,094 individuals with diabetes. Using equal weights for each country, diabetes prevalence was 9.0% (95% confidence interval [CI], 8.7-9.4), with 43.9% (95% CI, 41.9-45.9) reporting a prior diabetes diagnosis. Overall, 4.6% (95% CI, 3.9-5.4) of individuals with diabetes self-reported meeting need for all treatments recommended for them. Coverage of glucose-lowering medication was 50.5% (95% CI, 48.6-52.5); antihypertensive medication, 41.3% (95% CI, 39.3-43.3); cholesterol-lowering medication, 6.3% (95% CI, 5.5-7.2); diet counseling, 32.2% (95% CI, 30.7-33.7); exercise counseling, 28.2% (95% CI, 26.6-29.8); and weight-loss counseling, 31.5% (95% CI, 29.3-33.7). Countries at higher income levels tended to have greater coverage. Female sex and higher age, BMI, educational attainment, and household wealth were also associated with greater coverage.
Interpretation: Fewer than one in ten people with diabetes in LMICs receive coverage of guideline-based comprehensive diabetes treatment. Scaling-up the capacity of health systems to deliver treatment not only to lower glucose but also to address cardiovascular disease risk factors such as hypertension and high cholesterol are urgent global diabetes priorities.
Conflict of interest statement
Declaration of interests D.J.W. reports serving on a data-monitoring committee for Novo Nordisk.
Figures
Comment in
-
Gaps in achieving coverage of diabetes treatments in low-income and middle-income countries.Lancet Healthy Longev. 2021 Jun;2(6):e306-e307. doi: 10.1016/S2666-7568(21)00124-0. Epub 2021 Jun 3. Lancet Healthy Longev. 2021. PMID: 36098140 No abstract available.
References
-
- International Diabetes Federation. IDF Diabetes Atlas, 9th edition: International Diabetes Federation, 2019.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical