

Oral fosfomycin activity against Klebsiella pneumoniae in a dynamic bladder infection in vitro model
- PMID: 35211736
- PMCID: PMC9047678
- DOI: 10.1093/jac/dkac045
Oral fosfomycin activity against Klebsiella pneumoniae in a dynamic bladder infection in vitro model
Abstract
Introduction: The use of oral fosfomycin for urinary tract infections (UTIs) caused by non-Escherichia coli uropathogens is uncertain, including Klebsiella pneumoniae, the second most common uropathogen.
Methods: A multicompartment bladder infection in vitro model was used with standard media and synthetic human urine (SHU) to simulate urinary fosfomycin exposure after a single 3 g oral dose (fAUC0-72 16884 mg·h/L, t½ 5.5 h) against 15 K. pneumoniae isolates including ATCC 13883 (MIC 2 to >1024 mg/L) with a constant media inflow (20 mL/h) and 4-hourly voiding of each bladder. The impact of the media (CAMHB + G6P versus SHU) on fosfomycin MIC measurements, drug-free growth kinetics and regrowth after fosfomycin administration was assessed. A low and high starting inoculum (5.5 versus 7.5 log10 cfu/mL) was assessed in the bladder infection model.
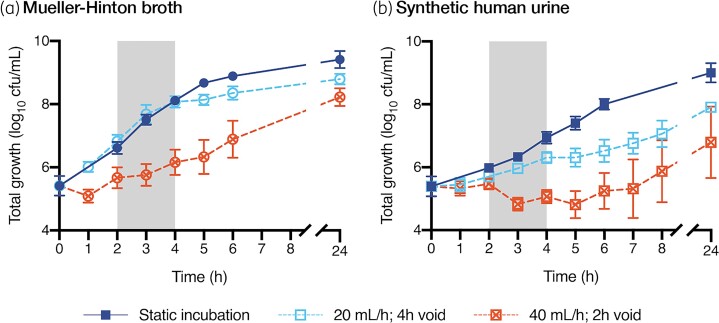
Results: Compared with CAMHB, isolates in SHU had a slower growth rate doubling time (37.7 versus 24.1 min) and reduced growth capacity (9.0 ± 0.3 versus 9.4 ± 0.3 log10 cfu/mL), which was further restricted with increased inflow rate (40 mL/h) and more frequent voids (2-hourly). Regrowth was commonly observed in both media with emergence of fosfomycin resistance promoted by a high starting inoculum in CAMHB (MIC rise to ≥1024 mg/L in 13/14 isolates). Resistance was rarely detected in SHU, even with a high starting inoculum (MIC rise to ≥1024 mg/L in 2/14 isolates).
Conclusions: Simulated in an in vitro UTI model, the regrowth of K. pneumoniae urinary isolates was inadequately suppressed following oral fosfomycin therapy. Efficacy was further reduced by a high starting inoculum.
© The Author(s) 2022. Published by Oxford University Press on behalf of British Society for Antimicrobial Chemotherapy.
Figures


Similar articles
-
Evaluation of pooled human urine and synthetic alternatives in a dynamic bladder infection in vitro model simulating oral fosfomycin therapy.J Microbiol Methods. 2020 Apr;171:105861. doi: 10.1016/j.mimet.2020.105861. Epub 2020 Feb 5. J Microbiol Methods. 2020. PMID: 32035114
-
Fosfomycin efficacy and emergence of resistance among Enterobacteriaceae in an in vitro dynamic bladder infection model.J Antimicrob Chemother. 2018 Mar 1;73(3):709-719. doi: 10.1093/jac/dkx441. J Antimicrob Chemother. 2018. PMID: 29253153
-
Impact of bacterial species and baseline resistance on fosfomycin efficacy in urinary tract infections.J Antimicrob Chemother. 2020 Apr 1;75(4):988-996. doi: 10.1093/jac/dkz519. J Antimicrob Chemother. 2020. PMID: 31873748
-
Fosfomycin trometamol: a review of its use as a single-dose oral treatment for patients with acute lower urinary tract infections and pregnant women with asymptomatic bacteriuria.Drugs. 2013 Nov;73(17):1951-66. doi: 10.1007/s40265-013-0143-y. Drugs. 2013. PMID: 24202878 Review.
-
Treatment of urinary tract infections in the era of antimicrobial resistance and new antimicrobial agents.Postgrad Med. 2020 Apr;132(3):234-250. doi: 10.1080/00325481.2019.1680052. Epub 2019 Oct 24. Postgrad Med. 2020. PMID: 31608743 Review.
Cited by
-
Impact of a Primary Care Antimicrobial Stewardship Program on Bacterial Resistance Control and Ecological Imprint in Urinary Tract Infections.Antibiotics (Basel). 2022 Dec 8;11(12):1776. doi: 10.3390/antibiotics11121776. Antibiotics (Basel). 2022. PMID: 36551433 Free PMC article.
-
Daily fosfomycin versus levofloxacin for complicated urinary tract infections.mBio. 2023 Oct 31;14(5):e0167723. doi: 10.1128/mbio.01677-23. Epub 2023 Sep 12. mBio. 2023. PMID: 37698412 Free PMC article.
-
Wild-Type Domestication: Loss of Intrinsic Metabolic Traits Concealed by Culture in Rich Media.Microb Ecol. 2024 Nov 21;87(1):144. doi: 10.1007/s00248-024-02459-z. Microb Ecol. 2024. PMID: 39567391 Free PMC article.
-
Oral ciprofloxacin biofilm activity in a catheter-associated urinary tract infection model.J Antimicrob Chemother. 2025 Feb 3;80(2):413-426. doi: 10.1093/jac/dkae424. J Antimicrob Chemother. 2025. PMID: 39626168 Free PMC article.
-
Dynamic In Vitro PK/PD Infection Models for the Development and Optimisation of Antimicrobial Regimens: A Narrative Review.Antibiotics (Basel). 2024 Dec 10;13(12):1201. doi: 10.3390/antibiotics13121201. Antibiotics (Basel). 2024. PMID: 39766591 Free PMC article. Review.
References
-
- Keijzers G, Macdonald SP, Udy AAet al. . The Australasian Resuscitation In Sepsis Evaluation: Fluids or vasopressors in emergency department sepsis (ARISE FLUIDS), a multi-centre observational study describing current practice in Australia and New Zealand. Emerg Med Australas 2020; 32: 586–98. - PMC - PubMed
-
- Bezabih YM, Sabiiti W, Alamneh Eet al. . The global prevalence and trend of human intestinal carriage of ESBL-producing Escherichia coli in the community. J Antimicrob Chemother 2021; 76: 22–9. - PubMed
-
- Quaegebeur A, Brunard L, Javaudin Fet al. . Trends and prediction of antimicrobial susceptibility in urinary bacteria isolated in European emergency departments: the EuroUTI 2010–16 Study. J Antimicrob Chemother 2019; 74: 3069–76. - PubMed
-
- Vardakas KZ, Legakis NJ, Triarides Net al. . Susceptibility of contemporary isolates to fosfomycin: a systematic review of the literature. Int J Antimicrob Agents 2016; 47: 269–85. - PubMed
-
- Zarakolu P, Eser OK, Otlu Bet al. . In-vitro activity of fosfomycin against Escherichia coli and Klebsiella pneumoniae bloodstream isolates and frequency of OXA-48, NDM, KPC, VIM, IMP types of carbapenemases in the carbapenem-resistant groups. J Chemother 2021; 1–6. 10.1080/1120009X.2021.1963618. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
