

Creatinine-based GFR-estimating equations in children with overweight and obesity
- PMID: 35211793
- PMCID: PMC9395456
- DOI: 10.1007/s00467-021-05396-y
Creatinine-based GFR-estimating equations in children with overweight and obesity
Abstract
Background: With the increasing prevalence of childhood obesity and related development of chronic kidney disease (CKD), there is a critical need to understand how best to assess kidney function in children with obesity. Since serum creatinine (SCr) is recommended as marker of first choice for GFR estimation, we evaluated and compared creatinine-based GFR equations in children with overweight and obesity.
Methods: Six hundred children with overweight and obesity (53.5% female; mean age 12.20 ± 3.28 years; mean BMI z-score 3.31 ± 0.75) were included from the Centre for Overweight Adolescent and Children's Healthcare (COACH).
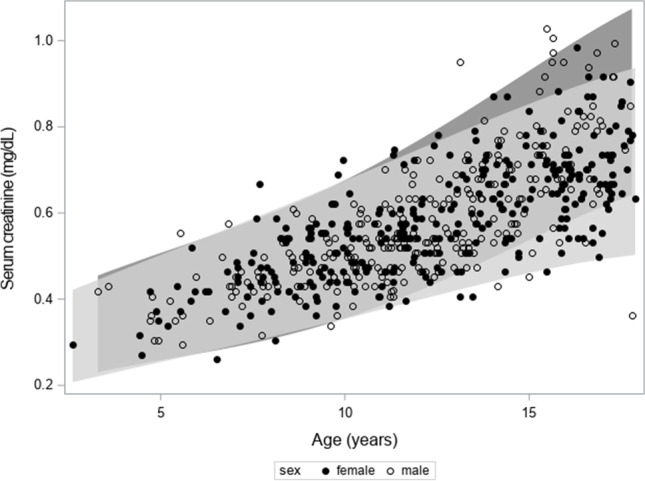
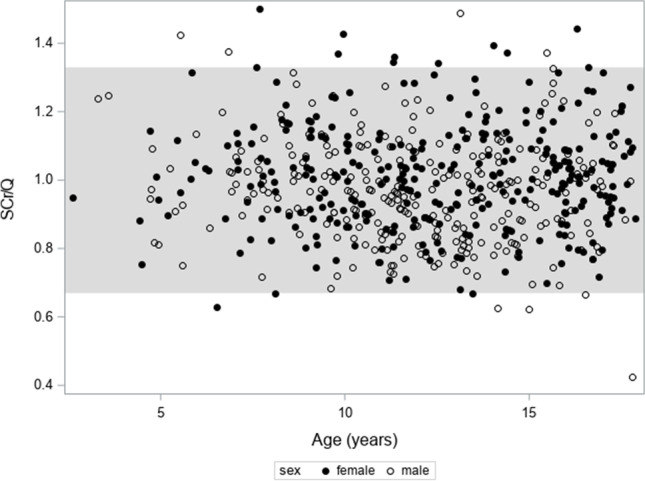
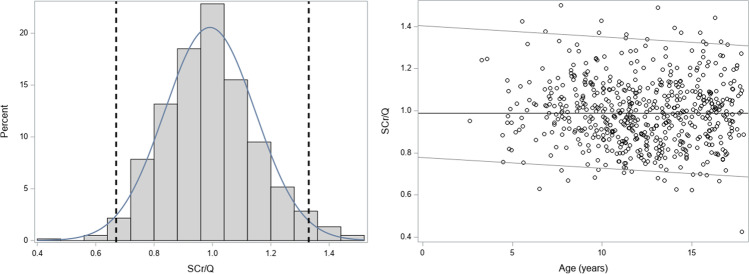
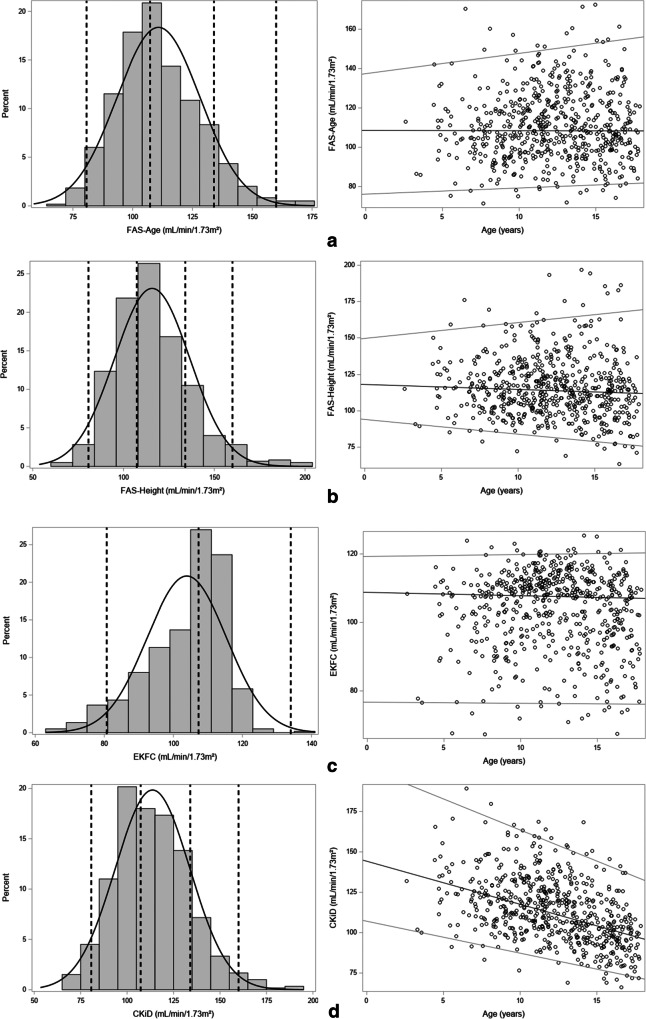
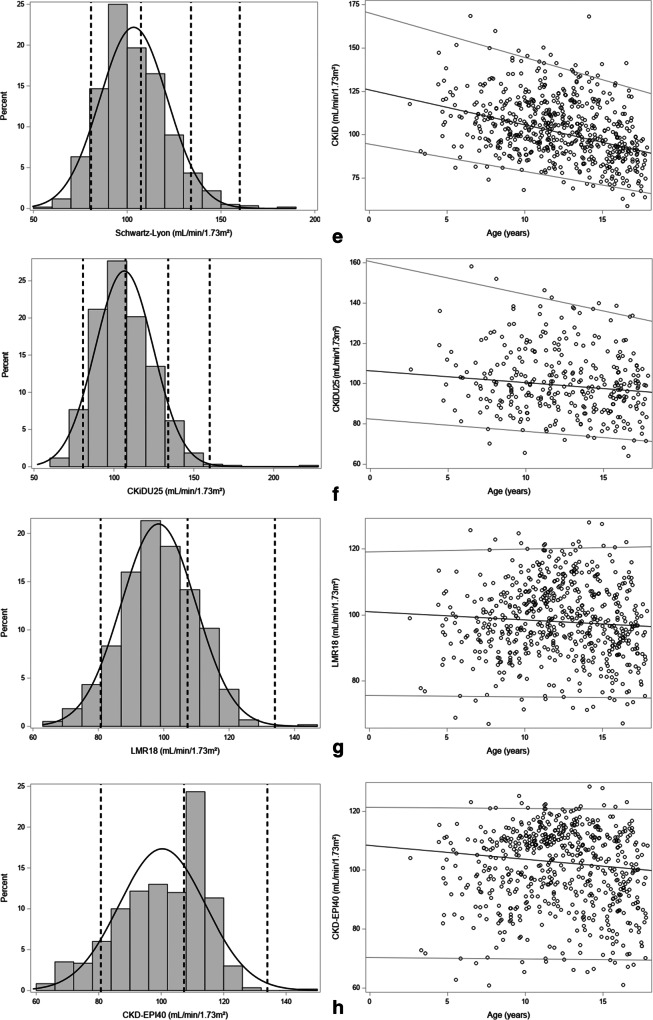
Results: Serum creatinine (SCr), normalized using Q-age polynomials obtained from reference values, results in median and mean SCr/Q value close to "1" for all age groups, and 96.5% of the children have a SCr/Q within the reference band [0.67-1.33], corresponding to the 2.5th and 97.5th percentile. eGFR CKiD (bedside Schwartz equation) and Schwartz-Lyon decreased with age, whereas eGFR EKFC and modified CKD-EPI40 showed no age-dependency, but the distribution of eGFR values was not symmetrical. eGFR CKiD under 25 (CKiDU25) demonstrated no age-dependency but major sex differences were observed. eGFR FAS age, FAS height, and adjusted-creatinine revised Lund-Malmö (LMR18) showed a relatively symmetrical distribution and no age-dependency.
Conclusions: Serum creatinine (SCr) values of children with overweight and obesity are mostly within the reference range for children. Normalization of SCr using reference Q-age polynomials works very well in this cohort. After evaluation of the different equations, we suggest that FAS age, FAS height, and LMR18 are the preferred creatinine-based GFR-estimating equations in children with overweight and obesity.
Clinicaltrial: gov; Registration Number: NCT02091544. A higher resolution version of the Graphical abstract is available as Supplementary information.
Keywords: Childhood obesity; Creatinine; Pediatrics; eGFR.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- López-Martínez M, Luis-Lima S, Morales E, Navarro-Díaz M, Negrín-Mena N, Folgueras T, Escamilla B, Estupiñán S, Delgado-Mallén P, Marrero-Miranda D, González-Rinne A, Miquel-Rodríguez RM, Cobo-Caso MA, Díaz-Martín L, Jiménez-Sosa A, González-Rinne F, Torres A, Porrini E. The estimation of GFR and the adjustment for BSA in overweight and obesity: a dreadful combination of two errors. Int J Obes (Lond) 2020;44:1129–1140. doi: 10.1038/s41366-019-0476-z. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
