

Not only a small liver - The pathologist's perspective in the pediatric liver transplant setting
- PMID: 35212319
- PMCID: PMC9040542
- DOI: 10.32074/1591-951X-753
Not only a small liver - The pathologist's perspective in the pediatric liver transplant setting
Abstract
Pediatric liver transplantation represents a safe and long-lasting treatment option for various disease types, requiring the pathologist's input. Indeed, an accurate and timely diagnosis is crucial in reporting and grading native liver diseases, evaluating donor liver eligibility and identifying signs of organ injury in the post-transplant follow-up. However, as the procedure is more frequently and widely performed, deceptive and unexplored histopathologic features have emerged with relevant consequences on patient management, particularly when dealing with long-term treatment and weaning of immunosuppression.
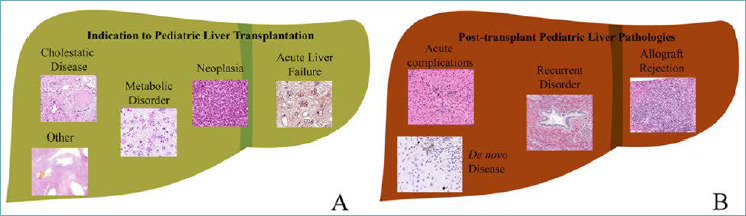
In this complex and challenging scenario, this review aims to depict the most relevant histopathologic conditions which could be encountered in pediatric liver transplantation. We will tackle the conditions representing the main indications for transplantation in childhood as well as the complications burdening the post-transplant phases, either immunologically (i.e., rejection) or non-immunologically mediated. Lastly, we hope to provide concise, yet significant, suggestions related to innovative pathology techniques in pediatric liver transplantation.
Keywords: acute complication; chronic complication; histopathology; next-generation pathology; pediatric liver transplantation.
Copyright © 2022 Società Italiana di Anatomia Patologica e Citopatologia Diagnostica, Divisione Italiana della International Academy of Pathology.
Conflict of interest statement
The Authors declare no conflict of interest.
Figures
Similar articles
-
Outcome of 200 Pediatric Living Donor Liver Transplantations in India.Indian Pediatr. 2017 Nov 15;54(11):913-918. doi: 10.1007/s13312-017-1181-4. Epub 2017 Aug 24. Indian Pediatr. 2017. PMID: 28849768
-
Liver transplantation. The pediatric challenge.Clin Liver Dis. 2000 Nov;4(4):879-927. doi: 10.1016/s1089-3261(05)70146-x. Clin Liver Dis. 2000. PMID: 11232362 Review.
-
Liver transplantation at the University of Chicago.Clin Transpl. 1995:187-97. Clin Transpl. 1995. PMID: 8794265
-
Thirty-five consecutive pediatric living donor liver transplantation: experiences and lessons learned from a single center.Hepatogastroenterology. 2014 Mar-Apr;61(130):391-7. Hepatogastroenterology. 2014. PMID: 24901148
-
De novo malignancies after liver transplantation: The effect of immunosuppression-personal data and review of literature.World J Gastroenterol. 2019 Sep 21;25(35):5356-5375. doi: 10.3748/wjg.v25.i35.5356. World J Gastroenterol. 2019. PMID: 31558879 Free PMC article.
Cited by
-
The Landscape of HNF1B Deficiency: A Syndrome Not Yet Fully Explored.Cells. 2023 Jan 13;12(2):307. doi: 10.3390/cells12020307. Cells. 2023. PMID: 36672242 Free PMC article. Review.
References
-
- Kwong AJ, Kim WR, Lake JR, et al. . OPTN/SRTR 2019 Annual Data Report: Liver. Am J Transplant. 2021;21 Suppl 2:208-315. https://doi.org/10.1111/ajt.16494 10.1111/ajt.16494 - DOI - PubMed
-
- de Ville de Goyet J, Baumann U, Karam V, et al. European Liver Intestine Transplant Association . European Liver Transplant Registry: donor and transplant surgery aspects of 16,641 liver transplantations in children. Hepatology 2022;75:634-645. https://doi.org/10.1002/hep.32223 10.1002/hep.32223 - DOI - PubMed
-
- Duffy JP, Kao K, Ko CY, et al. . Long-term patient outcome and quality of life after liver transplantation: analysis of 20-year survivors. Ann Surg 2010;252:652-661. https://doi.org/10.1097/SLA.0b013e3181f5f23a 10.1097/SLA.0b013e3181f5f23a - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
