

A Nationwide Analysis of Risk of Prostate Cancer Diagnosis and Mortality following an Initial Negative Transrectal Ultrasound Biopsy with Long-Term Followup
- PMID: 35212571
- PMCID: PMC9428937
- DOI: 10.1097/JU.0000000000002491
A Nationwide Analysis of Risk of Prostate Cancer Diagnosis and Mortality following an Initial Negative Transrectal Ultrasound Biopsy with Long-Term Followup
Abstract
Purpose: Magnetic resonance imaging (MRI) targeted prostate biopsy has been shown to find many high-grade prostate cancers in men with concurrent negative transrectal ultrasound (TRUS) systematic biopsy. The oncologic risk of such tumors can be explored by looking at long-term outcomes of men with negative TRUS biopsy followed without MRI. The aim was to analyze the mortality after initial and second negative TRUS biopsy.
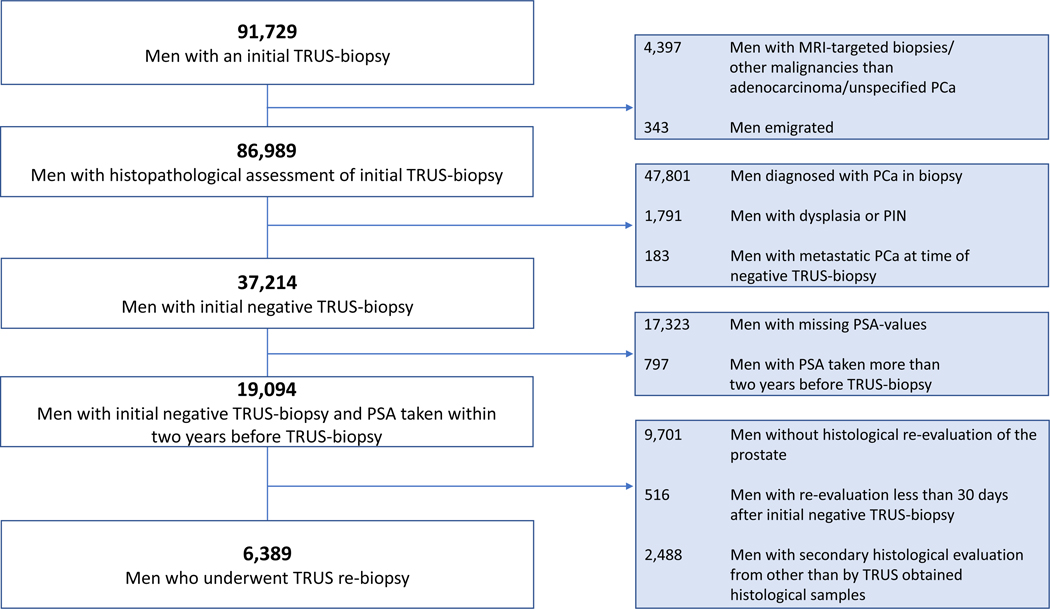
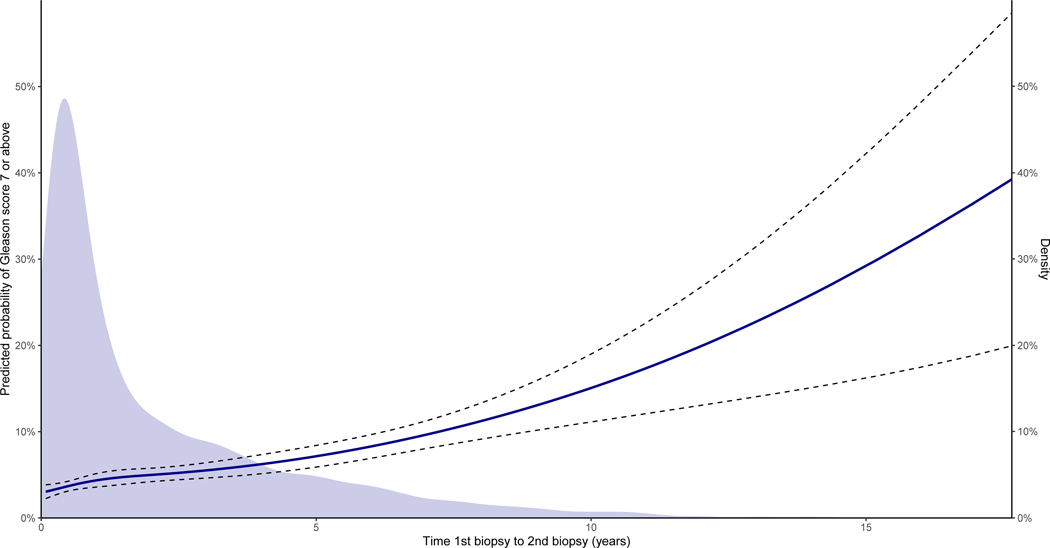
Materials and methods: All men who underwent initial TRUS biopsies between January 1, 1995 and December 31, 2016 in Denmark were included. A total of 37,214 men had a negative initial TRUS biopsy and 6,389 underwent a re-biopsy. Risk of cause-specific mortality was analyzed with competing risks. Diagnosis of Gleason score ≥7 prostate cancer following negative biopsies was analyzed with multivariable logistic regression including time to re-biopsy, prostate specific antigen (PSA), age and digital rectal examination.
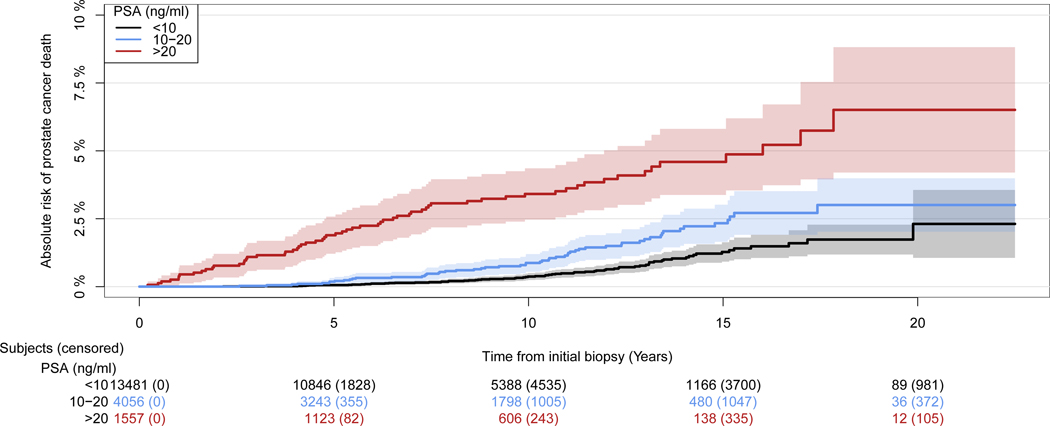
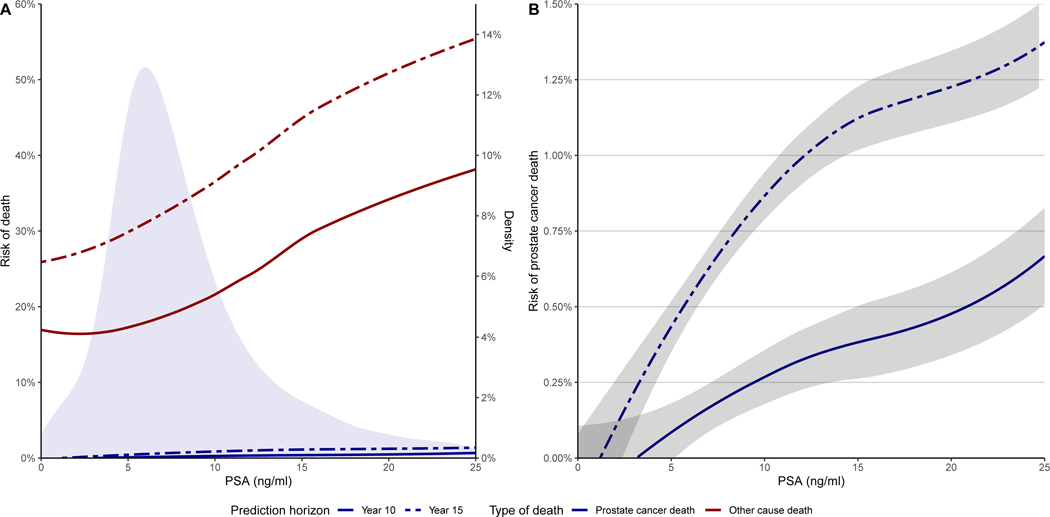
Results: The 15-year prostate cancer-specific mortality was 1.9% (95% CI: 1.7-2.1). Prostate cancer-specific mortality was 1.3% (95% CI: 0.9-1.6) and 4.6% (95% CI: 3.4-5.8) for men with PSA <10 and >20 ng/ml, respectively. Of the TRUS re-biopsies 12% were Gleason score ≥7 and risk of Gleason score ≥7 increased with longer time to re-biopsy (p <0.001). Mortality after re-biopsy was similar to after initial biopsy.
Conclusions: Men with negative TRUS biopsies have a very low prostate cancer-specific mortality, especially with PSA <10 ng/ml. This raises serious questions about the routine use of MRI targeting for initial prostate biopsy and suggests that MRI targeting should only be recommended for men with PSA >10 ng/ml after negative biopsy.
Keywords: biopsy; epidemiology; magnetic resonance imaging; mortality; prostatic neoplasm.
Conflict of interest statement
Conflict of interest. Andrew Vickers is named on a patent for a statistical method to detect prostate cancer, the 4Kscore, that has been commercialized by OPKO Health. Andrew Vickers receives royalties from sales of the test and has stock options in OPKO Health.
Figures
Comment in
-
A Nationwide Analysis of Risk of Prostate Cancer Diagnosis and Mortality following an Initial Negative Transrectal Ultrasound Biopsy with Long-Term Followup. Letter.J Urol. 2022 Jul;208(1):223. doi: 10.1097/JU.0000000000002700. Epub 2022 Apr 8. J Urol. 2022. PMID: 35394353 No abstract available.
-
Editorial Comment.J Urol. 2022 Jul;208(1):108. doi: 10.1097/JU.0000000000002491.02. Epub 2022 Apr 22. J Urol. 2022. PMID: 35450426 No abstract available.
-
Editorial Comment.J Urol. 2022 Jul;208(1):107-108. doi: 10.1097/JU.0000000000002491.01. Epub 2022 Apr 22. J Urol. 2022. PMID: 35450428 No abstract available.
-
Con: Magnetic Resonance Imaging Targeting Leads to Overtreatment of Prostate Cancer.J Urol. 2022 Aug;208(2):248-249. doi: 10.1097/JU.0000000000002777. Epub 2022 May 12. J Urol. 2022. PMID: 35549452 No abstract available.
References
-
- Nafie S, Wanis M and Khan M: The efficacy of transrectal ultrasound guided biopsy versus transperineal template biopsy of the prostate in diagnosing prostate cancer in men with previous negative transrectal ultrasound guided biopsy. Urol. J 2017; 14. - PubMed
-
- Abraham NE, Mendhiratta N and Taneja SS: Patterns of repeat prostate biopsy in contemporary clinical practice. J. Urol 2015; 193. - PubMed
-
- Djavan B, Ravery V, Zlotta A, et al.: Prospective evaluation of prostate cancer detected on biopsies 1, 2, 3 and 4: When should we stop? J. Urol 2001; 166. - PubMed
-
- Fütterer JJ, Briganti A, De Visschere P, et al.: Can Clinically Significant Prostate Cancer Be Detected with Multiparametric Magnetic Resonance Imaging? A Systematic Review of the Literature. Eur. Urol 2015; 68. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
