

Measurement of Severe Acute Respiratory Syndrome Coronavirus 2 Antigens in Plasma of Pediatric Patients With Acute Coronavirus Disease 2019 or Multisystem Inflammatory Syndrome in Children Using an Ultrasensitive and Quantitative Immunoassay
- PMID: 35213684
- PMCID: PMC8903440
- DOI: 10.1093/cid/ciac160
Measurement of Severe Acute Respiratory Syndrome Coronavirus 2 Antigens in Plasma of Pediatric Patients With Acute Coronavirus Disease 2019 or Multisystem Inflammatory Syndrome in Children Using an Ultrasensitive and Quantitative Immunoassay
Abstract
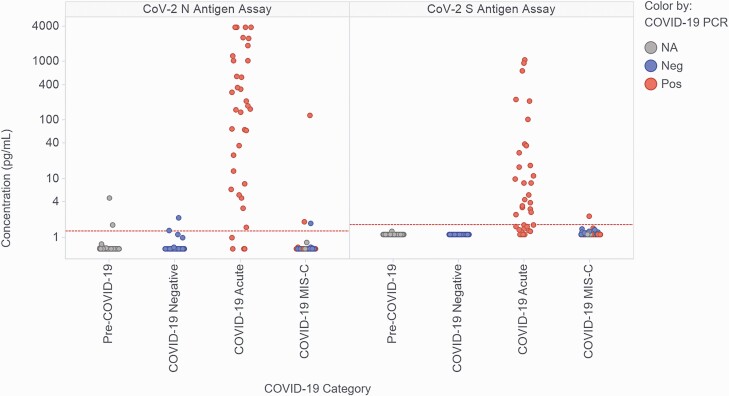
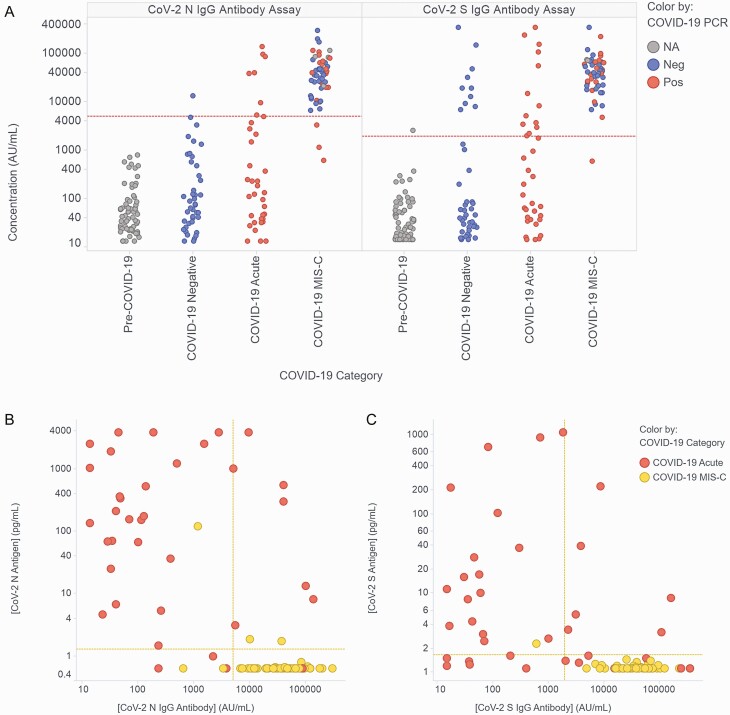
Background: Detection of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) antigens in blood has high sensitivity in adults with acute coronavirus disease 2019 (COVID-19), but sensitivity in pediatric patients is unclear. Recent data suggest that persistent SARS-CoV-2 spike antigenemia may contribute to multisystem inflammatory syndrome in children (MIS-C). We quantified SARS-CoV-2 nucleocapsid (N) and spike (S) antigens in blood of pediatric patients with either acute COVID-19 or MIS-C using ultrasensitive immunoassays (Meso Scale Discovery).
Methods: Plasma was collected from inpatients (<21 years) enrolled across 15 hospitals in 15 US states. Acute COVID-19 patients (n = 36) had a range of disease severity and positive nasopharyngeal SARS-CoV-2 RT-PCR within 24 hours of blood collection. Patients with MIS-C (n = 53) met CDC criteria and tested positive for SARS-CoV-2 (RT-PCR or serology). Controls were patients pre-COVID-19 (n = 67) or within 24 hours of negative RT-PCR (n = 43).
Results: Specificities of N and S assays were 95-97% and 100%, respectively. In acute COVID-19 patients, N/S plasma assays had 89%/64% sensitivity; sensitivities in patients with concurrent nasopharyngeal swab cycle threshold (Ct) ≤35 were 93%/63%. Antigen concentrations ranged from 1.28-3844 pg/mL (N) and 1.65-1071 pg/mL (S) and correlated with disease severity. In MIS-C, antigens were detected in 3/53 (5.7%) samples (3 N-positive: 1.7, 1.9, 121.1 pg/mL; 1 S-positive: 2.3 pg/mL); the patient with highest N had positive nasopharyngeal RT-PCR (Ct 22.3) concurrent with blood draw.
Conclusions: Ultrasensitive blood SARS-CoV-2 antigen measurement has high diagnostic yield in children with acute COVID-19. Antigens were undetectable in most MIS-C patients, suggesting that persistent antigenemia is not a common contributor to MIS-C pathogenesis.
Keywords: COVID-19; SARS-CoV-2; antigen; antigenemia; ultrasensitive immunoassay.
© The Author(s) 2022. Published by Oxford University Press for the Infectious Diseases Society of America. All rights reserved. For permissions, e-mail: journals.permissions@oup.com.
Conflict of interest statement
Potential conflicts of Interest . G. B. S., A. M., N. M., P. B, J. J., N. P., and D. R. are employees of Meso Scale Diagnostics. N. B. H. receives unrelated research support from Sanofi and Quidel. J. E. S. has received unrelated research support from Merck. H. R. F. is an Advisor for LuciraHealth. A. G. R. reports grants or contracts from National Institute of Allergy and Infectious Diseases to the institution outside of the submitted work; royalties or licenses from UpToDate for Pediatric Critical Care Section Editor; and is an unpaid Treasurer for International Sepsis Forum. All other authors report no potential conflicts. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.
Figures
Update of
-
Measurement of SARS-CoV-2 antigens in plasma of pediatric patients with acute COVID-19 or MIS-C using an ultrasensitive and quantitative immunoassay.medRxiv [Preprint]. 2021 Dec 9:2021.12.08.21267502. doi: 10.1101/2021.12.08.21267502. medRxiv. 2021. Update in: Clin Infect Dis. 2022 Oct 12;75(8):1351-1358. doi: 10.1093/cid/ciac160. PMID: 34909787 Free PMC article. Updated. Preprint.
References
-
- Centers for Disease Control and Prevention. Multisystem inflammatory syndrome in children (MIS-C) associated with coronavirus disease 2019 (COVID-19). Health Advisory. CDC Health Alert Network; May 14, 2020. Available at: https://emergency.cdc.gov/han/2020/han00432.asp. Accessed 12 January 2021.
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
