

Whole-Body Adaptive Functional Electrical Stimulation Kinesitherapy Can Promote the Restoring of Physiological Muscle Synergies for Neurological Patients
- PMID: 35214345
- PMCID: PMC8877830
- DOI: 10.3390/s22041443
Whole-Body Adaptive Functional Electrical Stimulation Kinesitherapy Can Promote the Restoring of Physiological Muscle Synergies for Neurological Patients
Abstract
Background: Neurological diseases and traumas are major factors that may reduce motor functionality. Functional electrical stimulation is a technique that helps regain motor function, assisting patients in daily life activities and in rehabilitation practices. In this study, we evaluated the efficacy of a treatment based on whole-body Adaptive Functional Electrical Stimulation Kinesitherapy (AFESK™) with the use of muscle synergies, a well-established method for evaluation of motor coordination. The evaluation is performed on retrospectively gathered data of neurological patients executing whole-body movements before and after AFESK-based treatments.
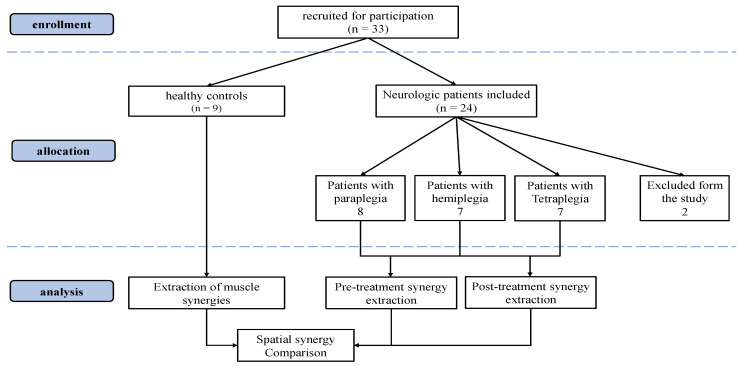
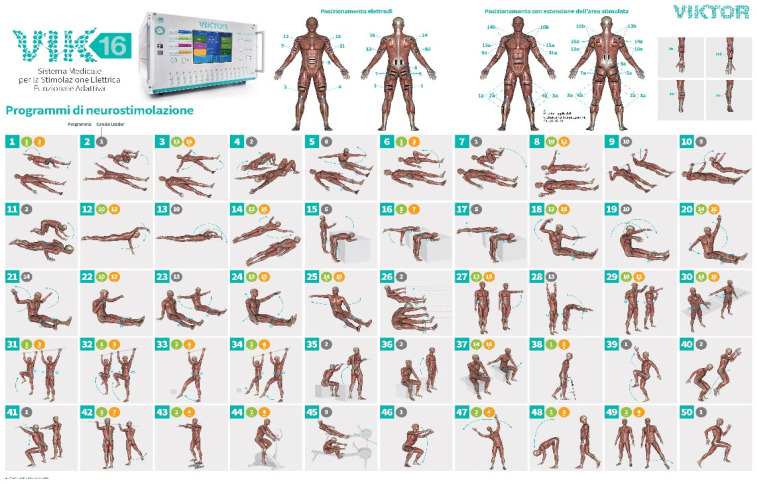
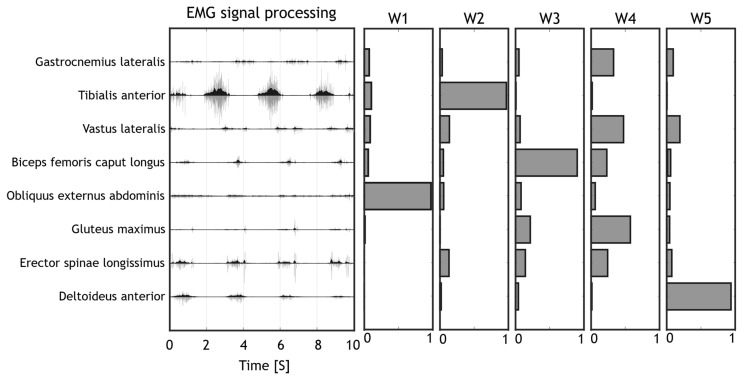
Methods: Twenty-four chronic neurologic patients and 9 healthy subjects were recruited in this study. The patient group was further subdivided in 3 subgroups: hemiplegic, tetraplegic and paraplegic. All patients underwent two acquisition sessions: before treatment and after a FES based rehabilitation treatment at the VIKTOR Physio Lab. Patients followed whole-body exercise protocols tailored to their needs. The control group of healthy subjects performed all movements in a single session and provided reference data for evaluating patients' performance. sEMG was recorded on relevant muscles and muscle synergies were extracted for each patient's EMG data and then compared to the ones extracted from the healthy volunteers. To evaluate the effect of the treatment, the motricity index was measured and patients' extracted synergies were compared to the control group before and after treatment.
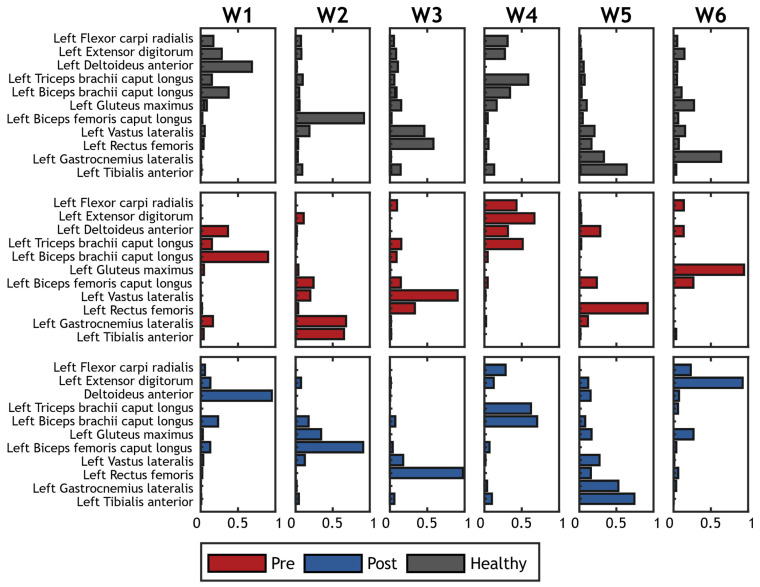
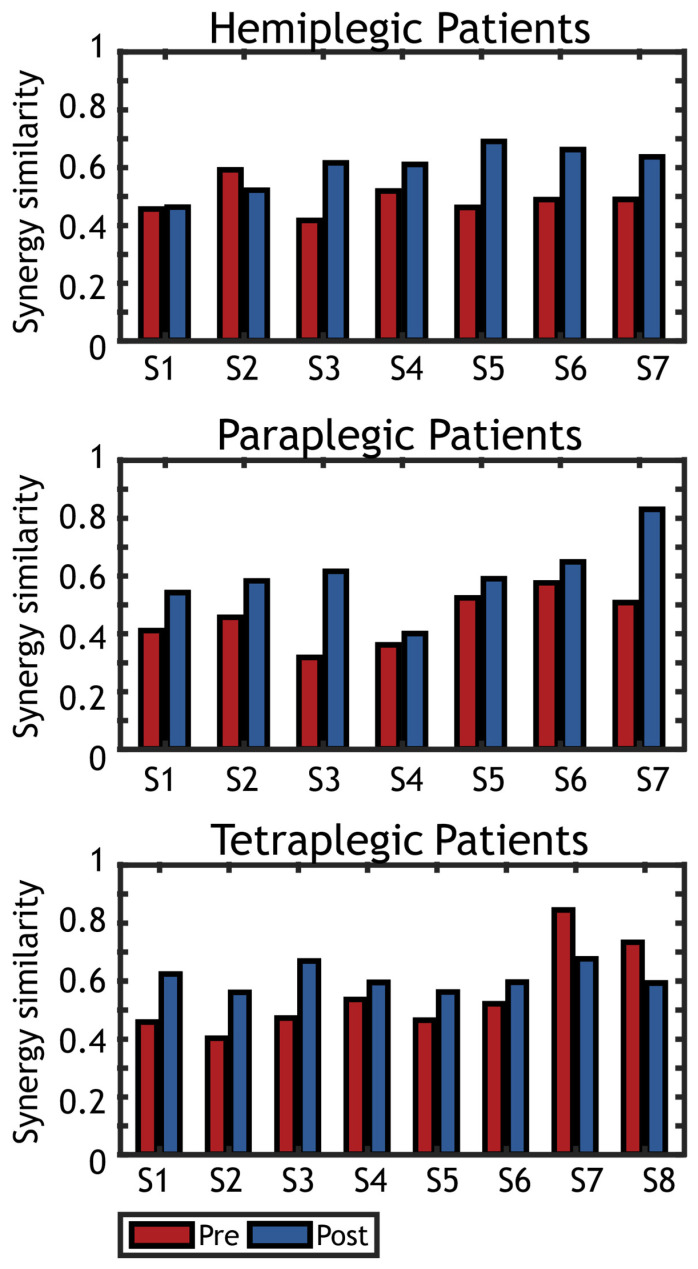
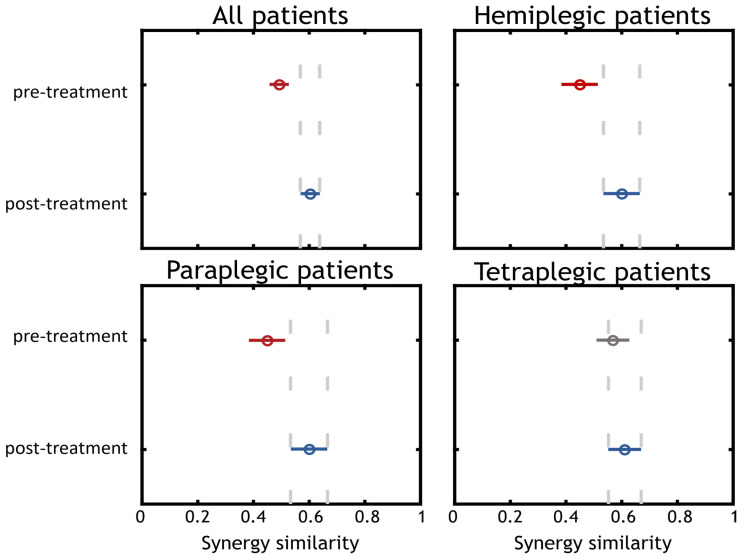
Results: After the treatment, patients' motricity index increased for many of the screened body segments. Muscle synergies were more similar to those of healthy people. Globally, the normalized synergy similarity in respect to the control group was 0.50 before the treatment and 0.60 after (p < 0.001), with improvements for each subgroup of patients.
Conclusions: AFESK treatment induced favorable changes in muscle activation patterns in chronic neurologic patients, partially restoring muscular patterns similar to healthy people. The evaluation of the synergic relationships of muscle activity when performing test exercises allows to assess the results of rehabilitation measures in patients with impaired locomotor functions.
Keywords: muscle synergies; neurological patients; whole body FES.
Conflict of interest statement
Viktor Terekhov and Guido Gabbrielli have interests in the exploitation of the AFESK technology: they are shareholders and respectively Chief scientific officer and Chief technology officer of VIKTOR S.r.l.
Figures


Similar articles
-
Evidence of synergy coordination patterns of upper-limb motor control in stroke patients with mild and moderate impairment.Front Physiol. 2023 Sep 11;14:1214995. doi: 10.3389/fphys.2023.1214995. eCollection 2023. Front Physiol. 2023. PMID: 37753453 Free PMC article.
-
A Personalized Multi-Channel FES Controller Based on Muscle Synergies to Support Gait Rehabilitation after Stroke.Front Neurosci. 2016 Sep 16;10:425. doi: 10.3389/fnins.2016.00425. eCollection 2016. Front Neurosci. 2016. PMID: 27695397 Free PMC article.
-
Alterations in intermuscular coordination underlying isokinetic exercise after a stroke and their implications on neurorehabilitation.J Neuroeng Rehabil. 2021 Jul 3;18(1):110. doi: 10.1186/s12984-021-00900-9. J Neuroeng Rehabil. 2021. PMID: 34217328 Free PMC article.
-
Neurorehabilitation with new functional electrical stimulation for hemiparetic upper extremity in stroke patients.J Nippon Med Sch. 2008 Feb;75(1):4-14. doi: 10.1272/jnms.75.4. J Nippon Med Sch. 2008. PMID: 18360073 Review.
-
Recent developments in muscle synergy analysis in young people with neurodevelopmental diseases: A Systematic Review.Front Bioeng Biotechnol. 2023 Apr 27;11:1145937. doi: 10.3389/fbioe.2023.1145937. eCollection 2023. Front Bioeng Biotechnol. 2023. PMID: 37180039 Free PMC article. Review.
Cited by
-
Biomedical Sensors for Functional Mapping: Techniques, Methods, Experimental and Medical Applications.Sensors (Basel). 2023 Aug 10;23(16):7063. doi: 10.3390/s23167063. Sensors (Basel). 2023. PMID: 37631600 Free PMC article.
-
The Number and Structure of Muscle Synergies Depend on the Number of Recorded Muscles: A Pilot Simulation Study with OpenSim.Sensors (Basel). 2022 Nov 8;22(22):8584. doi: 10.3390/s22228584. Sensors (Basel). 2022. PMID: 36433182 Free PMC article.
-
Improvement of Motor Imagination and Manual Ability Through Virtual Reality and Selective and Nonselective Functional Electrical Stimulation: Protocol for a Randomized Controlled Trial.JMIR Res Protoc. 2024 Nov 22;13:e63329. doi: 10.2196/63329. JMIR Res Protoc. 2024. PMID: 39576986 Free PMC article.
References
-
- Ebels P. EUObserver. Oct 22, 2012. [(accessed on 13 September 2021)]. Available online: https://euobserver.com/search?query=Disability+in+figures.
-
- Eurostat Population Structure and Ageing. Statistics Explained. 2019. [(accessed on 13 September 2021)]. Available online: https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Popul....
-
- World Health Organization World Health Organization: Rehabilitation. Jul 16, 2021. [(accessed on 14 September 2021)]. Available online: https://www.who.int/news-room/fact-sheets/detail/rehabilitation.
-
- Eurostat Healthcare Expenditure Statistics. 2021. [(accessed on 10 September 2021)]. Available online: https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Healt....
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
