

Evaluation of Serological Markers in Alveolar Echinococcosis Emphasizing the Correlation of PET-CTI Tracer Uptake with RecEm18 and Echinococcus-Specific IgG
- PMID: 35215182
- PMCID: PMC8880252
- DOI: 10.3390/pathogens11020239
Evaluation of Serological Markers in Alveolar Echinococcosis Emphasizing the Correlation of PET-CTI Tracer Uptake with RecEm18 and Echinococcus-Specific IgG
Abstract
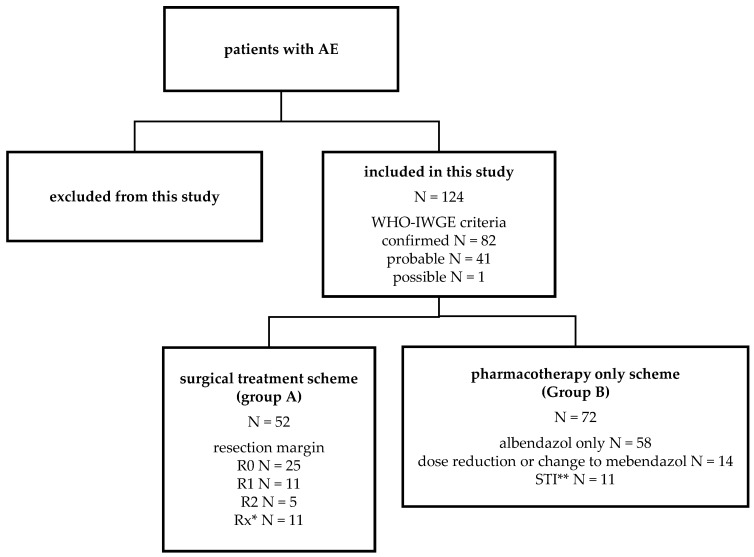
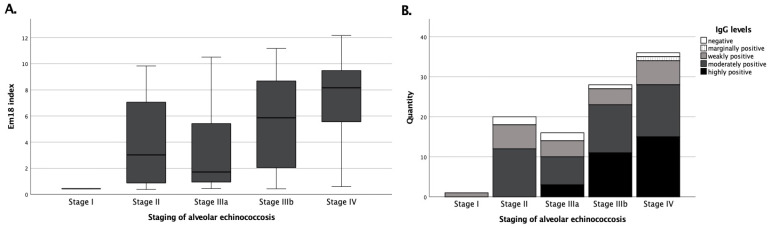
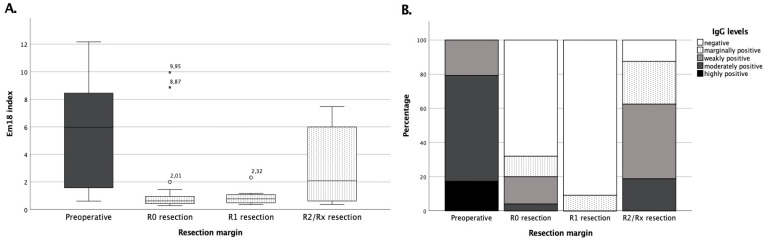
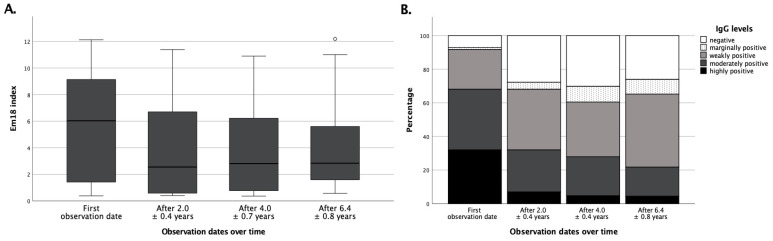
Human alveolar echinococcosis (AE), which is caused by the cestode Echinococcus (E.) multilocularis, is an epidemiologically relevant issue in modern medicine and still poses a diagnostic and therapeutic challenge. Since diagnosis mainly relies on imaging procedures and serological testing, we retrospectively and comparatively analyzed the performance of an Echinococcus IgG screening ELISA, whole serum IgE, and two specific confirmatory ELISA platforms using the defined E. multilocularis antigens Em2-Em18 (Em2+) and recombinant Em18 (recEm18). With special emphasis on the clinical usefulness of recEm18, we correlated the laboratory results with clinical characteristics and imaging findings in a large and well-characterized cohort of N = 124 AE patients, who were followed over several years after either surgical plus subsequent pharmacological treatment or pharmacotherapy alone. All patients had routinely received PET-CTI every two years. Our data reveal strong correlations for both Echinococcus IgG and recEm18 with tracer uptake in PET-CTI and parasitic lesion size and number, suggesting additional clinical usefulness of recEm18 for certain constellations only, while IgG and Em2+ still appear reasonable and sensitive screening methods for initial diagnosis of AE. With this study, we aim to contribute to further optimizing medical care of AE patients. For instance, it might be reasonable to consider the replacement of some PET-CTI follow-ups by imaging procedures with less radiation exposure or serological means alone. Further studies that clarify the correlation of serological markers with ultrasound criteria might be particularly useful, and further retrospective as well as prospective investigations are justified in this context.
Keywords: Echinococcus IgG; PET-CTI; alveolar echinococcosis; recEm18.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Gruener B., Kern P., Mayer B., Graeter T., Hillenbrand A., Barth T.E.F., Muche R., Henne-Bruns D., Kratzer W., Kern P. Comprehensive diagnosis and treatment of alveolar echinococcosis: A single-center, long-term observational study of 312 patients in Germany. GMS Infect. Dis. 2017;5:Doc01. doi: 10.3205/id000027. - DOI - PMC - PubMed
-
- Reinehr M., Micheloud C., Grimm F., Kronenberg P.A., Grimm J., Beck A., Nell J., Meyer zu Schwabedissen C., Furrer E., Muellhaupt B., et al. Pathology of echinococcosis: A morphologic and immunohistochemical study on 138 specimens with focus on the differential diagnosis between cystic and alveolar Echinococcosis. Am. J. Surg. Pathol. 2020;44:43–54. doi: 10.1097/PAS.0000000000001374. - DOI - PubMed
LinkOut - more resources
Full Text Sources
