Applying Zinc Nutrient Reference Values as Proposed by Different Authorities Results in Large Differences in the Estimated Prevalence of Inadequate Zinc Intake by Young Children and Women and in Cameroon
- PMID: 35215534
- PMCID: PMC8879783
- DOI: 10.3390/nu14040883
Applying Zinc Nutrient Reference Values as Proposed by Different Authorities Results in Large Differences in the Estimated Prevalence of Inadequate Zinc Intake by Young Children and Women and in Cameroon
Abstract
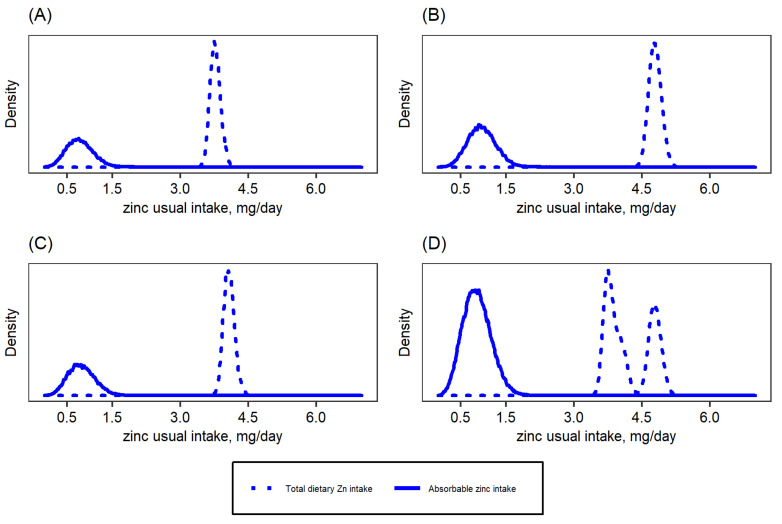
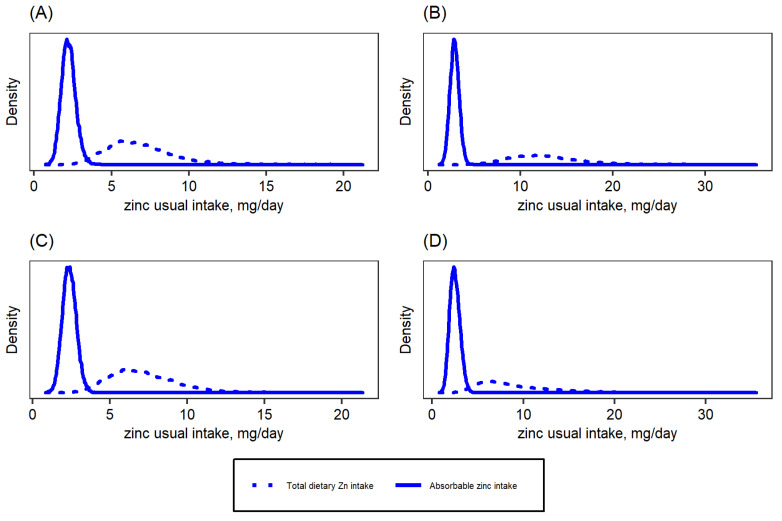
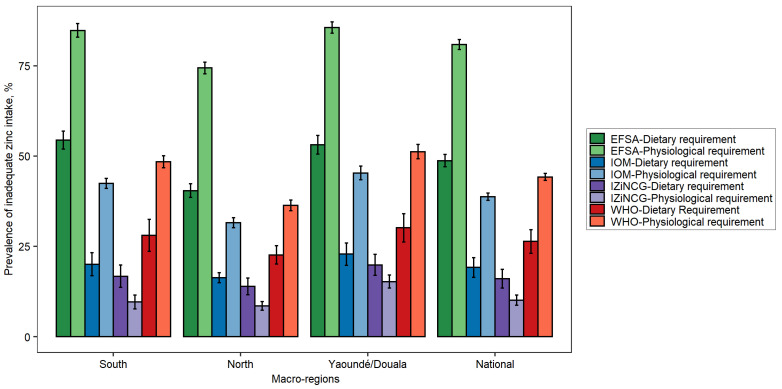
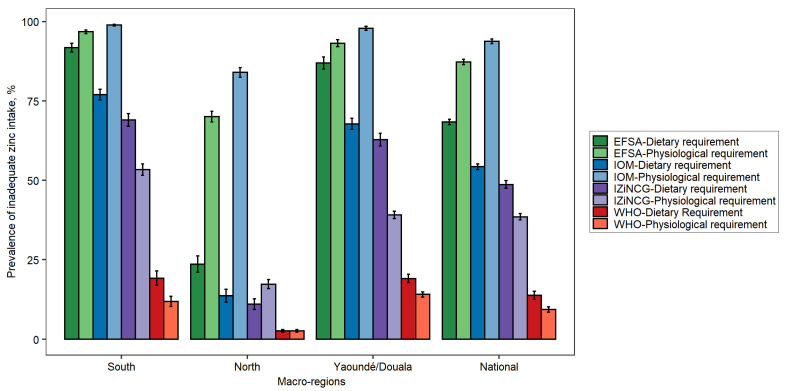
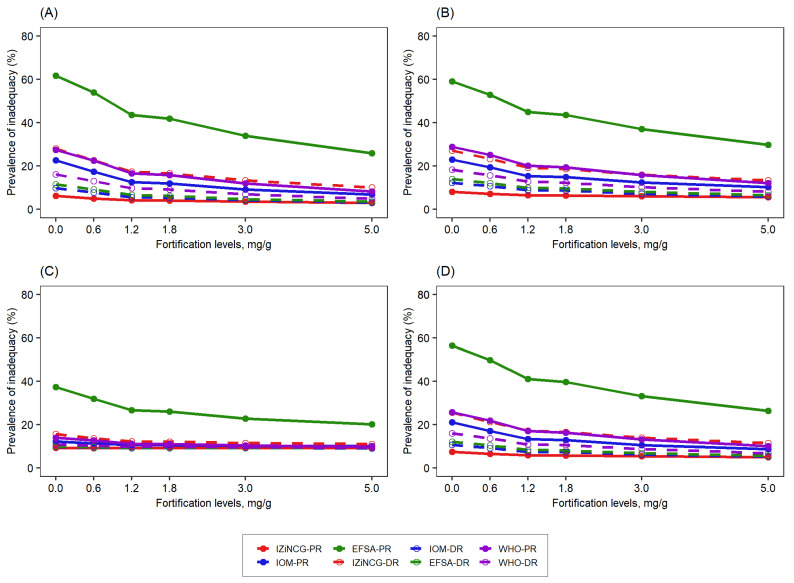
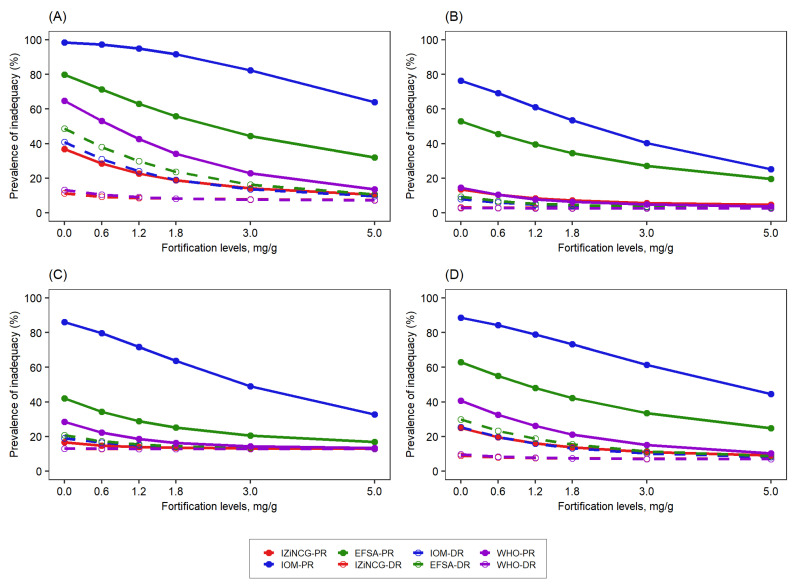
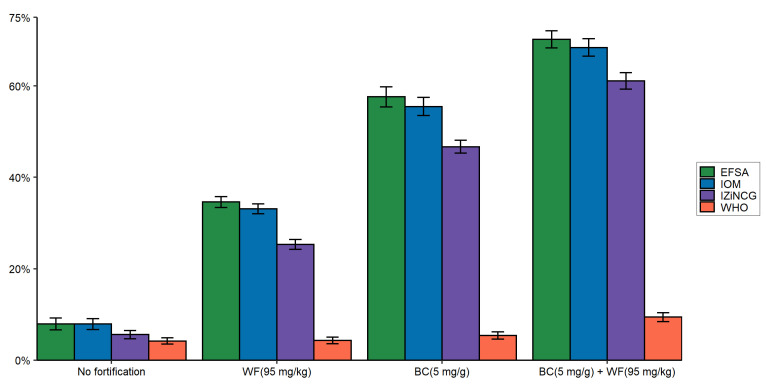
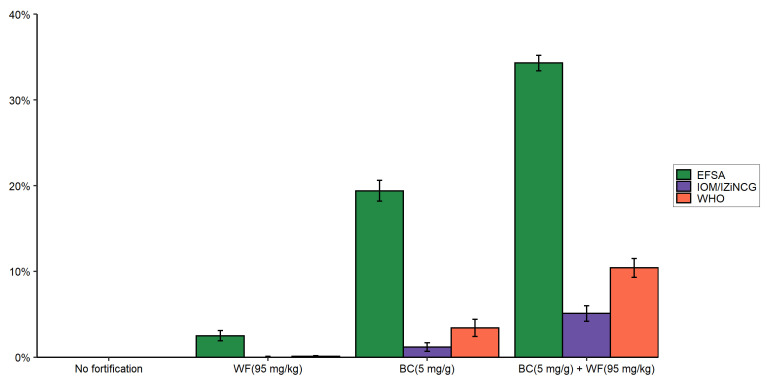
Nutrient reference values (NRVs) for zinc set by several expert groups differ widely and may affect the predicted prevalence of inadequate zinc intake. We examined this possibility using NRVs published by four different authorities and nationally representative dietary intake data collected among children aged 12-59 months and women in Cameroon. Usual zinc intake was estimated from 24 h recall data using the National Cancer Institute method. Prevalences of total zinc intake below the dietary requirement and of "absorbable zinc intake" below the physiological requirement were estimated using NRVs published by the World Health Organization (WHO), US Institute of Medicine (IOM), International Zinc Nutrition Consultative Group (IZiNCG), and European Food Safety Authority (EFSA). The prevalence of inadequate zinc intake ranged from 10% (IZiNCG-physiological requirement, 95% CI 7-13%) to 81% (EFSA-physiological requirement, 95% CI 78-84%) among children and 9% (WHO-physiological requirement, 95% CI 8-11.0%) to 94% (IOM-physiological requirement, 95% CI 92-95%) among women These differences in the prevalence of inadequate intake translated into sizeable differences in the predicted benefit and cost-effectiveness of zinc fortification programs. Depending on the NRVs applied, assessments differ regarding the need for and design of zinc fortification programs. Efforts are needed to harmonize NRVs for zinc.
Keywords: Cameroon; children; dietary assessment; fortification; modeling; women; zinc.
Conflict of interest statement
The authors declare no conflict of interest.
Figures