

Bypass Grafting and Native Coronary Artery Disease Activity
- PMID: 35216930
- PMCID: PMC9246289
- DOI: 10.1016/j.jcmg.2021.11.030
Bypass Grafting and Native Coronary Artery Disease Activity
Abstract
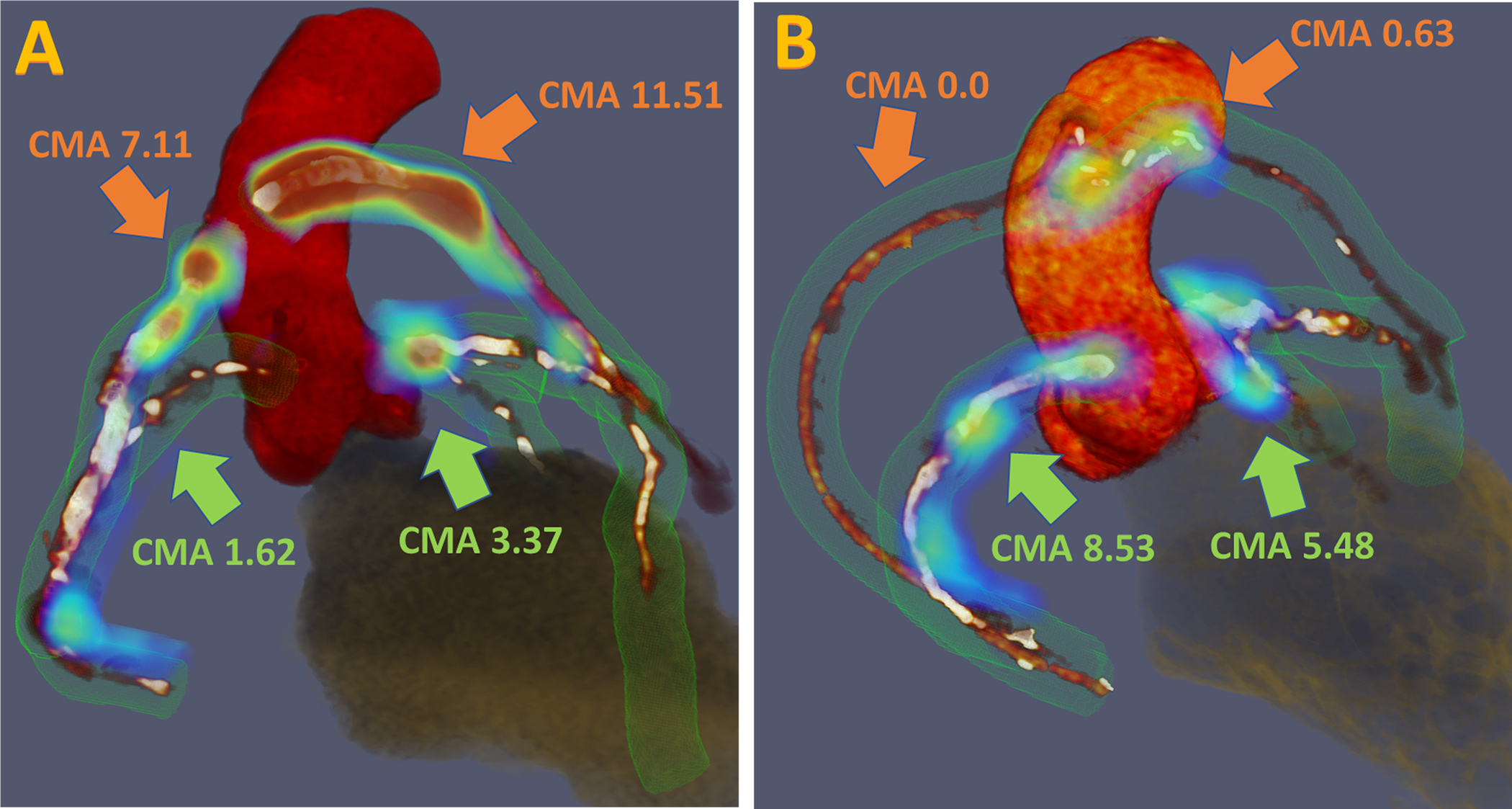
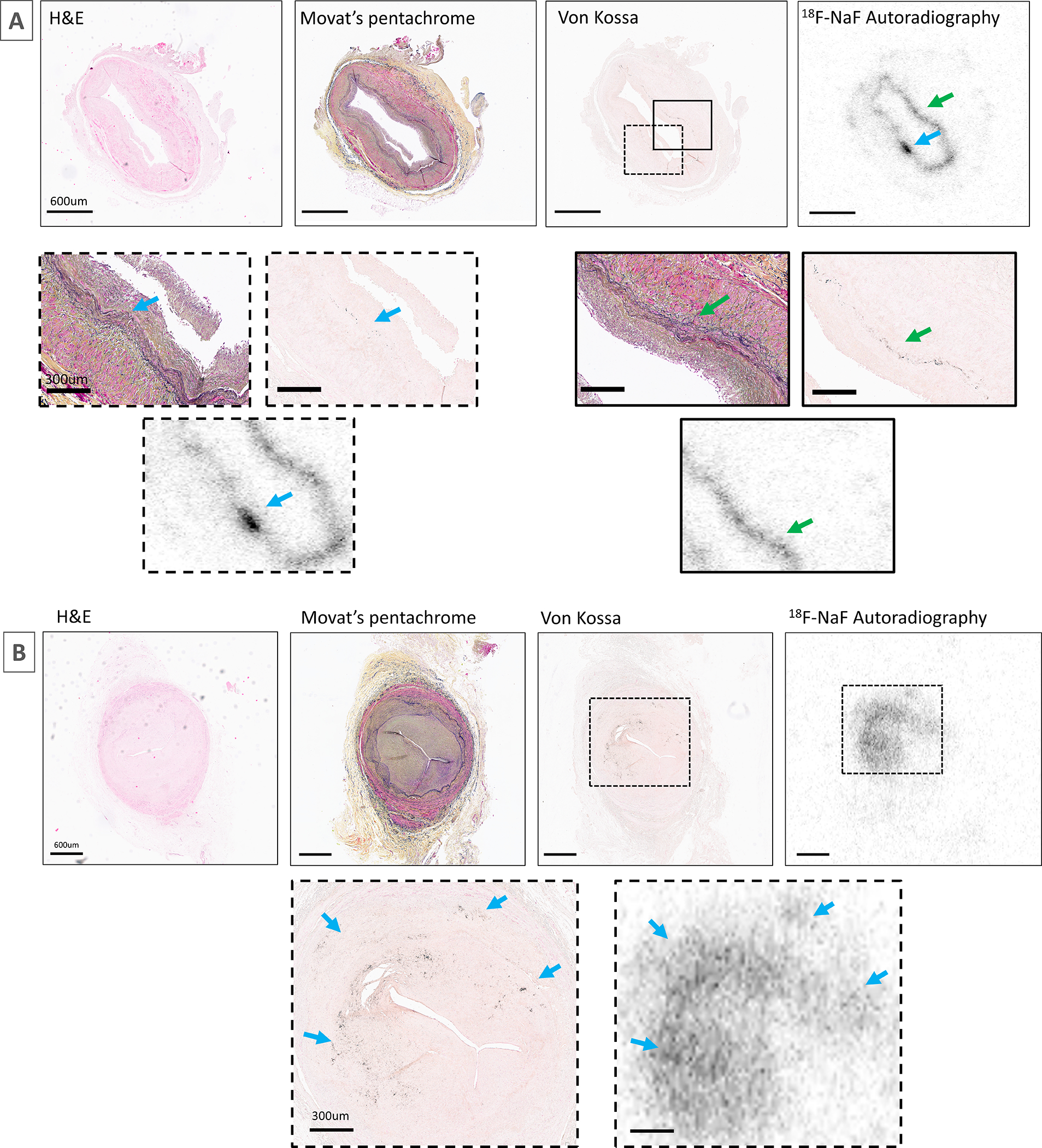
Objectives: The aim of this study was to describe the potential of 18F-sodium fluoride (18F-NaF) positron emission tomography (PET) to identify graft vasculopathy and to investigate the influence of coronary artery bypass graft (CABG) surgery on native coronary artery disease activity and progression.
Background: As well as developing graft vasculopathy, CABGs have been proposed to accelerate native coronary atherosclerosis.
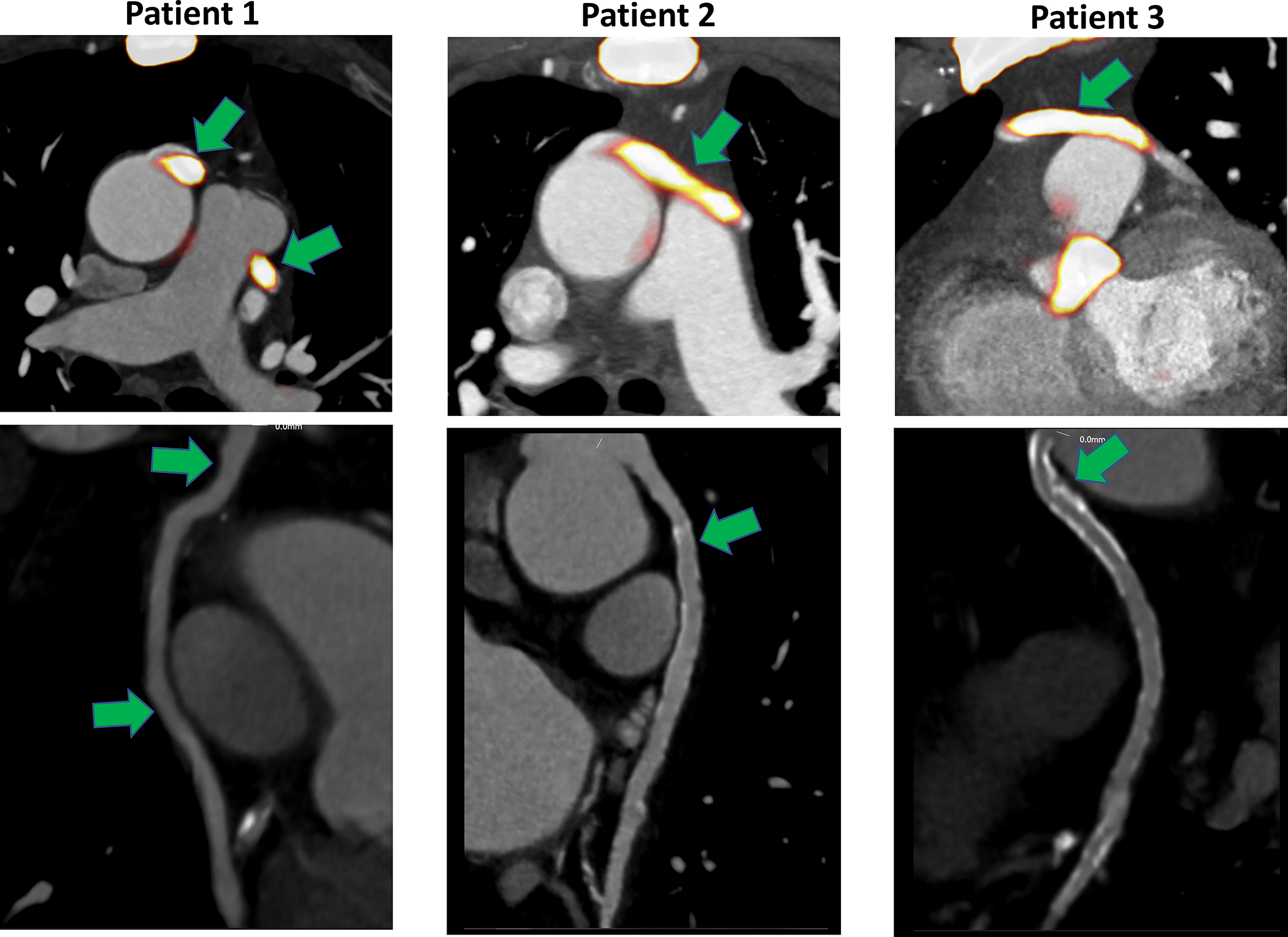
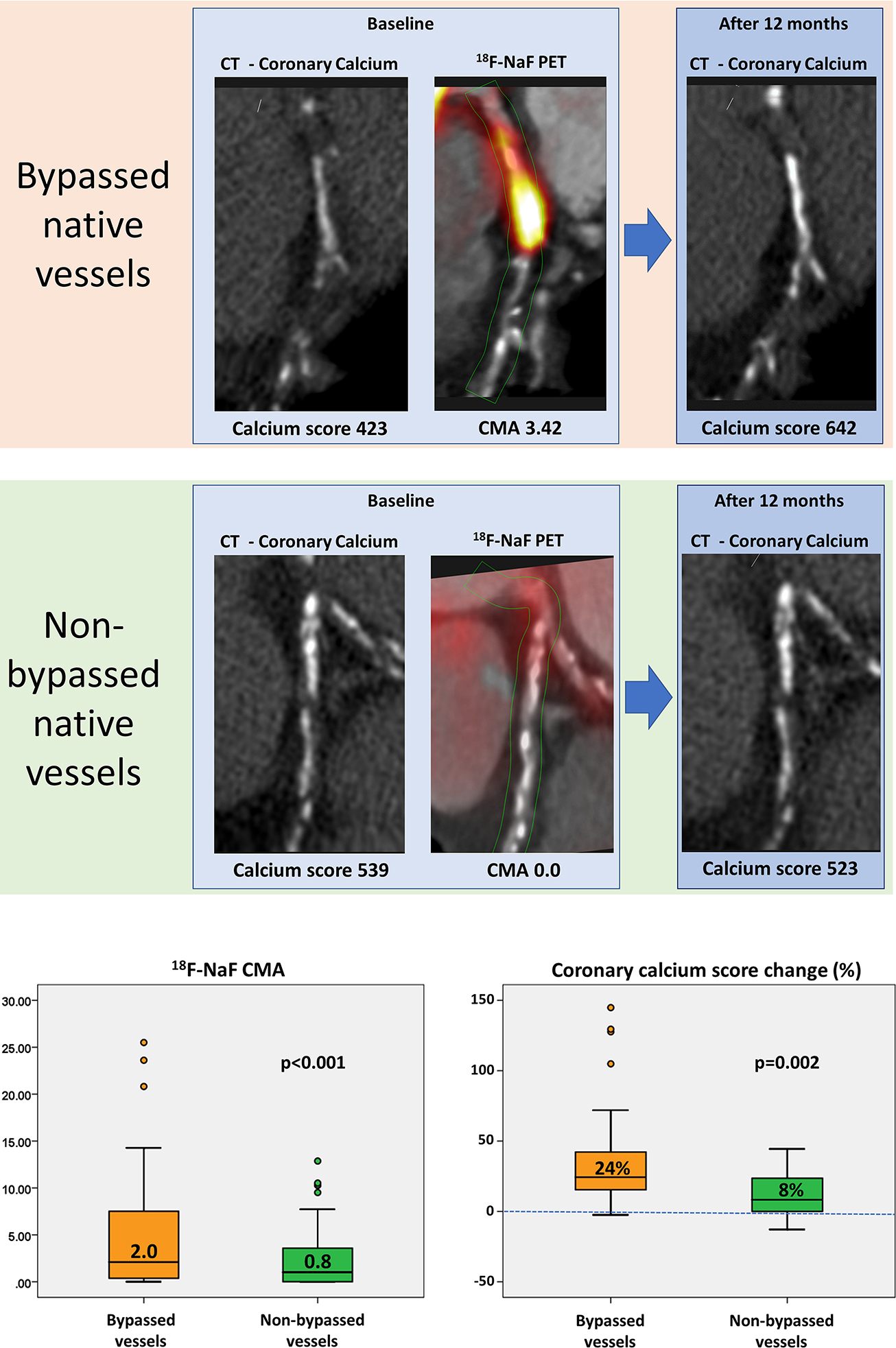
Methods: Patients with established coronary artery disease underwent baseline 18F-NaF PET, coronary artery calcium scoring, coronary computed tomographic angiography, and 1-year repeat coronary artery calcium scoring. Whole-vessel coronary microcalcification activity (CMA) on 18F-NaF PET and change in calcium scores were quantified in patients with and without CABG surgery.
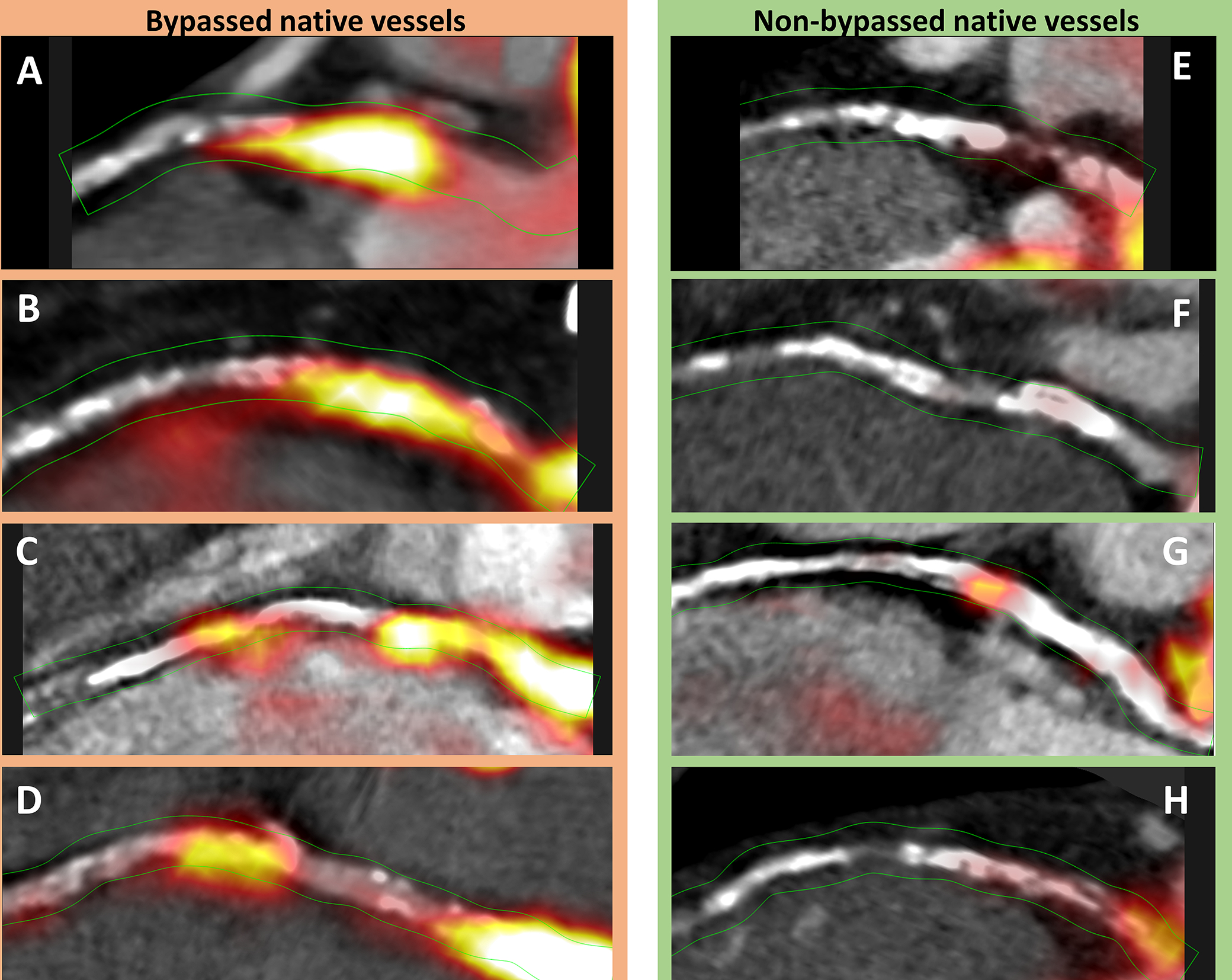
Results: Among 293 participants (mean age 65 ± 9 years, 84% men), 48 (16%) underwent CABG surgery 2.7 years [IQR: 1.4-10.4 years] previously. Although all arterial and the majority (120 of 128 [94%]) of vein grafts showed no 18F-NaF uptake, 8 saphenous vein grafts in 7 subjects had detectable CMA. Bypassed native coronary arteries had 3 times higher CMA values (2.1 [IQR: 0.4-7.5] vs 0.6 [IQR: 0-2.7]; P < 0.001) and greater progression of 1-year calcium scores (118 Agatston unit [IQR: 48-194 Agatston unit] vs 69 [IQR: 21-142 Agatston unit]; P = 0.01) compared with patients who had not undergone CABG, an effect confined largely to native coronary plaques proximal to the graft anastomosis. In sensitivity analysis, bypassed native coronary arteries had higher CMA (2.0 [IQR: 0.4-7.5] vs 0.8 [IQR: 0.3-3.2]; P < 0.001) and faster disease progression (24% [IQR: 16%-43%] vs 8% [IQR: 0%-24%]; P = 0.002) than matched patients (n = 48) with comparable burdens of coronary artery disease and cardiovascular comorbidities in the absence of bypass grafting.
Conclusions: Native coronary arteries that have been bypassed demonstrate increased disease activity and more rapid disease progression than nonbypassed arteries, an observation that appears independent of baseline atherosclerotic plaque burden. Microcalcification activity is not a dominant feature of graft vasculopathy.
Keywords: (18)F-NaF; CABG; PET/CT; coronary artery bypass graft; coronary artery disease.
Copyright © 2022 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Funding Support and Author Disclosures This research was supported in part by grant R01HL135557 from the National Heart, Lung, and Blood Institute. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. Dr Newby (CH/09/002, RE/18/5/34216, RG/16/10/32375), Dr Tzolos (FS/CRTF/20/24086), Dr Fletcher (FS/19/15/34155), Dr Baker (RG/20/5/34796), Dr Dweck (FS/14/78/31020), and Dr Williams (FS/ICRF/20/26002) are supported by the British Heart Foundation. Dr Adamson is supported by a Heart Foundation of New Zealand Senior Fellowship (1844). Dr van Beek is supported by the Scottish Imaging Network. Dr Tzolos was supported by a grant from the Dr Miriam and Sheldon G. Adelson Medical Research Foundation. Dr Newby is a recipient of a Wellcome Trust Senior Investigator Award (WT103782AIA). Dr Dweck is a recipient of the Sir Jules Thorn Award for Biomedical Research Award (2015). Dr Sellers is supported by fellowships from the Canadian Institutes of Health Research and the Michael Smith Foundation for Health Research. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
Comment in
-
Multimodal Imaging Insights Into Graft Vasculopathy and Progression of Native CAD Following CABG.JACC Cardiovasc Imaging. 2022 May;15(5):888-890. doi: 10.1016/j.jcmg.2022.01.018. JACC Cardiovasc Imaging. 2022. PMID: 35512959 Free PMC article. No abstract available.
References
-
- Goldman S, Zadina K, Moritz T, et al. Long-term patency of saphenous vein and left internal mammary artery grafts after coronary artery bypass surgery: Results from a Department of Veterans Affairs Cooperative Study. J Am Coll Cardiol 2004;44:2149–2156. - PubMed
-
- Fitzgibbon GM, Kafka HP, Leach AJ, Keon WJ, Hooper GD, Burton JR. Coronary bypass graft fate and patient outcome: Angiographic follow-up of 5,065 grafts related to survival and reoperation in 1,388 patients during 25 years. J Am Coll Cardiol 1996;28:616–626. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
