

Lack of association between pandemic chilblains and SARS-CoV-2 infection
- PMID: 35217624
- PMCID: PMC8892496
- DOI: 10.1073/pnas.2122090119
Lack of association between pandemic chilblains and SARS-CoV-2 infection
Abstract
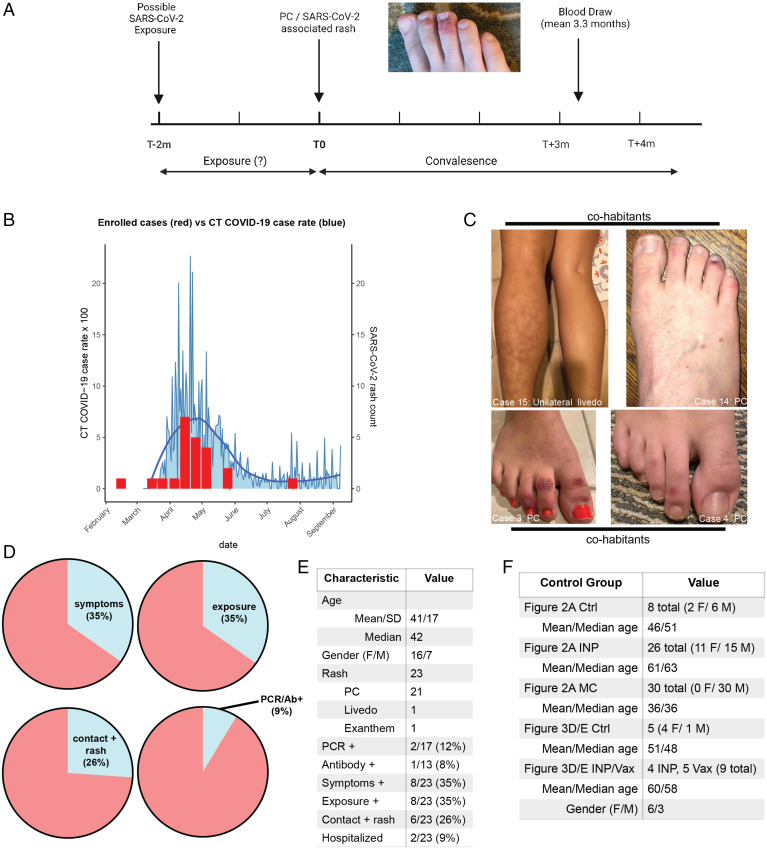
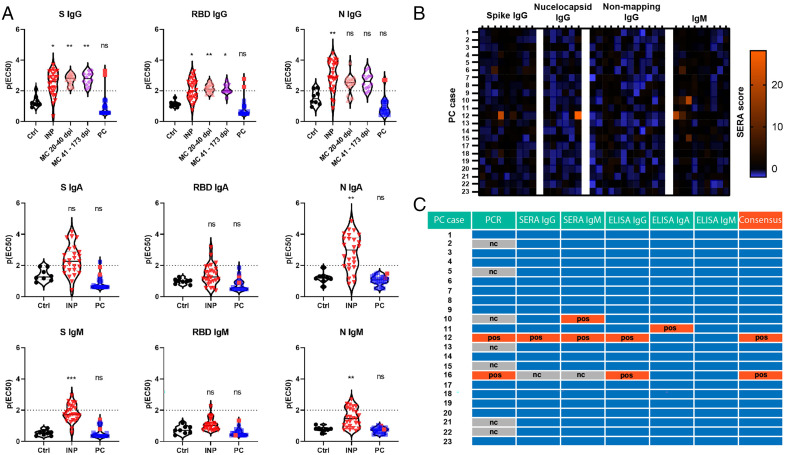
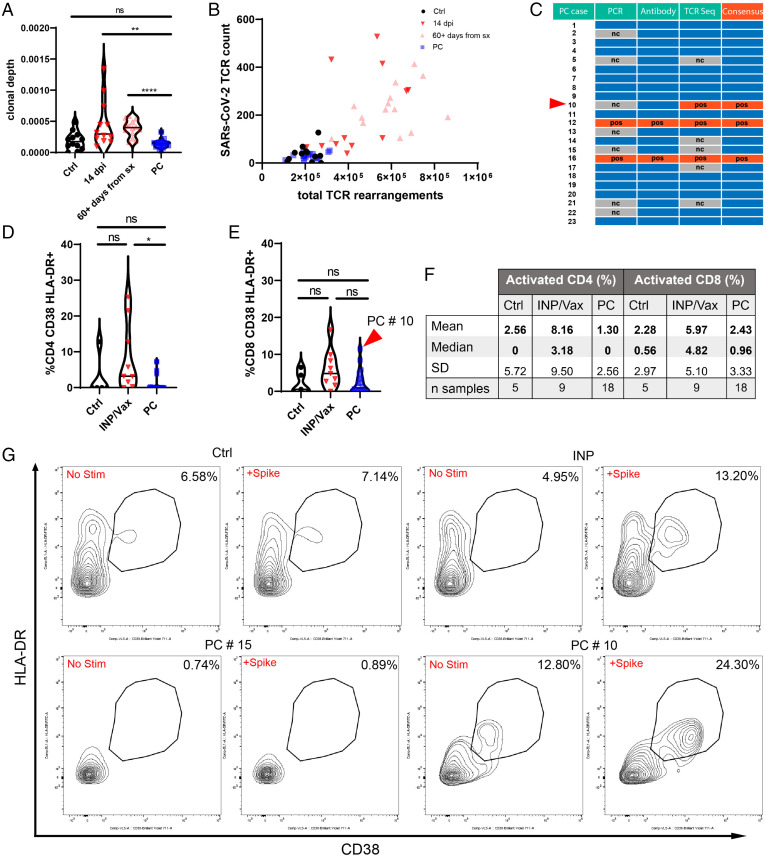
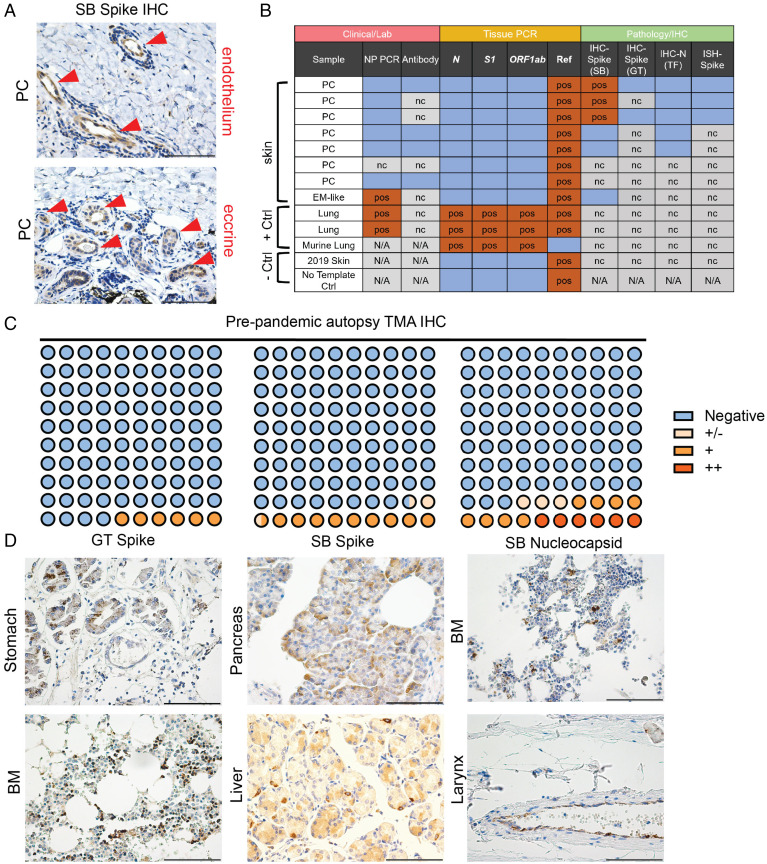
An increased incidence of chilblains has been observed during the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) pandemic and attributed to viral infection. Direct evidence of this relationship has been limited, however, as most cases do not have molecular evidence of prior SARS-CoV-2 infection with PCR or antibodies. We enrolled a cohort of 23 patients who were diagnosed and managed as having SARS-CoV-2-associated skin eruptions (including 21 pandemic chilblains [PC]) during the first wave of the pandemic in Connecticut. Antibody responses were determined through endpoint titration enzyme-linked immunosorbent assay and serum epitope repertoire analysis. T cell responses to SARS-CoV-2 were assessed by T cell receptor sequencing and in vitro SARS-CoV-2 antigen-specific peptide stimulation assays. Immunohistochemical and PCR studies of PC biopsies and tissue microarrays for evidence of SARS-CoV-2 were performed. Among patients diagnosed and managed as "covid toes" during the pandemic, we find a percentage of prior SARS-CoV-2 infection (9.5%) that approximates background seroprevalence (8.5%) at the time. Immunohistochemistry studies suggest that SARS-CoV-2 staining in PC biopsies may not be from SARS-CoV-2. Our results do not support SARS-CoV-2 as the causative agent of pandemic chilblains; however, our study does not exclude the possibility of SARS-CoV-2 seronegative abortive infections.
Keywords: SARS-CoV-2; chilblain; covid toe; interferon; pernio.
Copyright © 2022 the Author(s). Published by PNAS.
Conflict of interest statement
The authors declare no competing interest.
Figures
Comment in
-
Are 'COVID toes' actually caused by the coronavirus?Nature. 2022 Mar;603(7903):779. doi: 10.1038/d41586-022-00707-1. Nature. 2022. PMID: 35296839 No abstract available.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
