

Point-of-care anti-CD19 CAR T-cells for treatment of relapsed and refractory aggressive B-cell lymphoma
- PMID: 35218999
- PMCID: PMC9519531
- DOI: 10.1016/j.jtct.2022.02.017
Point-of-care anti-CD19 CAR T-cells for treatment of relapsed and refractory aggressive B-cell lymphoma
Abstract
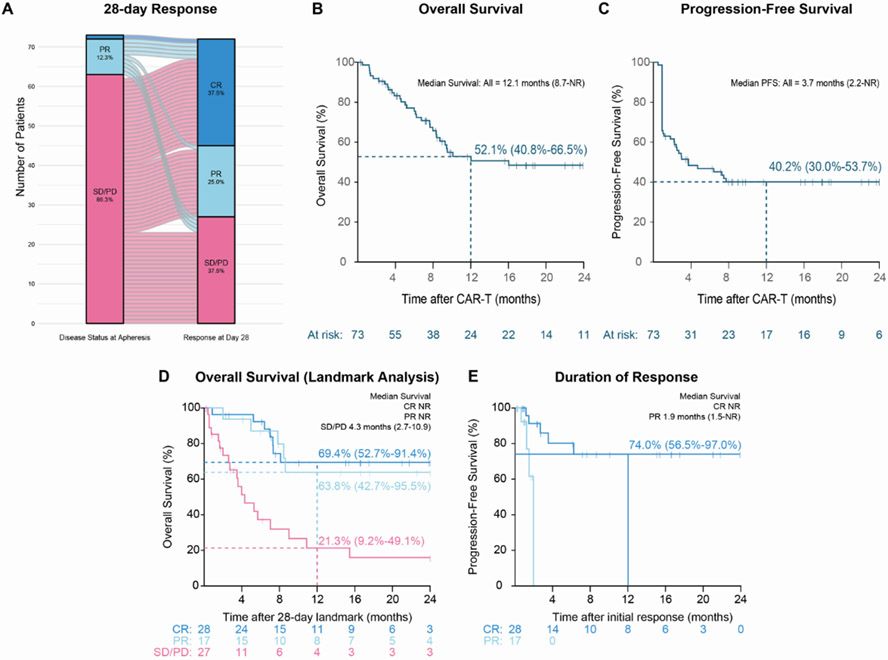
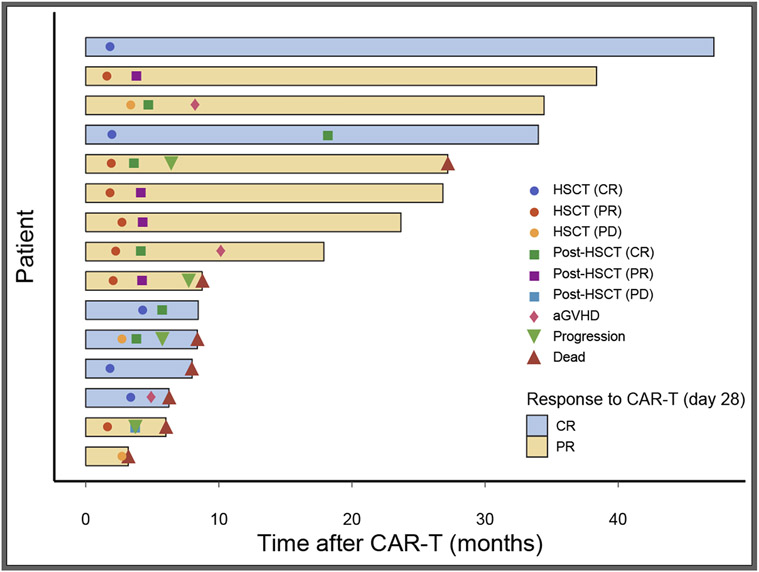
Anti CD19 chimeric antigen receptor (CAR) T-cell therapy has transformed the care of relapsed and refractory aggressive B-cell lymphoma. However, financial toxicity and manufacturing time represent barriers to its widespread implementation. Study applicability, toxicity, and efficacy of a locally produced autologous CD19-directed CAR T-cell product were studied. We performed a phase 1b/2 clinical trial with a point-of-care (POC) CAR T-cell product that contains a CD28 costimulatory domain. Adult patients with aggressive B-cell lymphoma or transformed low-grade lymphoma who received at least 2 prior regimens were eligible. A total of 73 patients, with a median age of 49 years, met inclusion criteria. CAR T-cell production time from apheresis was 10 days (interquartile range 10-11), negating the need for bridging chemotherapy. Overall and complete response rates were 62.5% and 37.5%. Median progression-free and overall survival were 3.7 and 12.1 months, respectively. Overall and progression-free survival at 12 months were 52.1% (confidence interval [CI]: 40.8%-66.5%) and 40% (CI: 30%-53.7%), respectively. Patients who achieved response had longer progression-free and overall survival. Grade 3-4 cytokine release syndrome was observed in 9.5% of the patients, and immune effector cell-associated neurotoxicity syndrome grade 3-4 in 21.9%. No deaths occurred due to CAR T-cell toxicity. Fifteen patients (20%) underwent allogeneic stem cell transplantation at a median time of 60 days after CAR T-cell therapy; 8 were alive at last follow-up. Of the 6 patients who underwent the transplantation in complete response 2 deceased because of toxicity. POC CAR T-cells are a feasible therapeutic option in aggressive B-cell lymphoma. They provide good efficacy while minimizing production time and the need for bridging therapy.
Keywords: Aggressive B-cell lymphoma; Allogeneic stem cell transplantation; CAR T-cell; Point of care.
Copyright © 2022 The American Society for Transplantation and Cellular Therapy. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflict of Interest
None
Figures
Comment in
-
Bench at Bedside Models Facilitate CAR-T Cell Supply Chain.Transplant Cell Ther. 2022 May;28(5):221-222. doi: 10.1016/j.jtct.2022.04.005. Transplant Cell Ther. 2022. PMID: 35523472 No abstract available.
References
-
- Hagberg H, Gisselbrecht C, CORAL study group. Randomised phase III study of R-ICE versus R-DHAP in relapsed patients with CD20 diffuse large B-cell lymphoma (DLBCL) followed by high-dose therapy and a second randomisation to maintenance treatment with rituximab or not: an update of the CORAL study. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol 2006;17 Suppl 4(suppl 4):iv31–2. - PubMed
-
- Schuster SJ, Bishop MR, Tam CS, et al. Tisagenlecleucel in Adult Relapsed or Refractory Diffuse Large B-Cell Lymphoma. N. Engl. J. Med 2019;380(1):45–56. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
