

Variation in the COVID-19 infection-fatality ratio by age, time, and geography during the pre-vaccine era: a systematic analysis
- PMID: 35219376
- PMCID: PMC8871594
- DOI: 10.1016/S0140-6736(21)02867-1
Variation in the COVID-19 infection-fatality ratio by age, time, and geography during the pre-vaccine era: a systematic analysis
Erratum in
-
Department of Error.Lancet. 2022 Apr 16;399(10334):1468. doi: 10.1016/S0140-6736(22)00666-3. Lancet. 2022. PMID: 35430020 Free PMC article. No abstract available.
Abstract
Background: The infection-fatality ratio (IFR) is a metric that quantifies the likelihood of an individual dying once infected with a pathogen. Understanding the determinants of IFR variation for COVID-19, the disease caused by the SARS-CoV-2 virus, has direct implications for mitigation efforts with respect to clinical practice, non-pharmaceutical interventions, and the prioritisation of risk groups for targeted vaccine delivery. The IFR is also a crucial parameter in COVID-19 dynamic transmission models, providing a way to convert a population's mortality rate into an estimate of infections.
Methods: We estimated age-specific and all-age IFR by matching seroprevalence surveys to total COVID-19 mortality rates in a population. The term total COVID-19 mortality refers to an estimate of the total number of deaths directly attributable to COVID-19. After applying exclusion criteria to 5131 seroprevalence surveys, the IFR analyses were informed by 2073 all-age surveys and 718 age-specific surveys (3012 age-specific observations). When seroprevalence was reported by age group, we split total COVID-19 mortality into corresponding age groups using a Bayesian hierarchical model to characterise the non-linear age pattern of reported deaths for a given location. To remove the impact of vaccines on the estimated IFR age pattern, we excluded age-specific observations of seroprevalence and deaths that occurred after vaccines were introduced in a location. We estimated age-specific IFR with a non-linear meta-regression and used the resulting age pattern to standardise all-age IFR observations to the global age distribution. All IFR observations were adjusted for baseline and waning antibody-test sensitivity. We then modelled age-standardised IFR as a function of time, geography, and an ensemble of 100 of the top-performing covariate sets. The covariates included seven clinical predictors (eg, age-standardised obesity prevalence) and two measures of health system performance. Final estimates for 190 countries and territories, as well as subnational locations in 11 countries and territories, were obtained by predicting age-standardised IFR conditional on covariates and reversing the age standardisation.
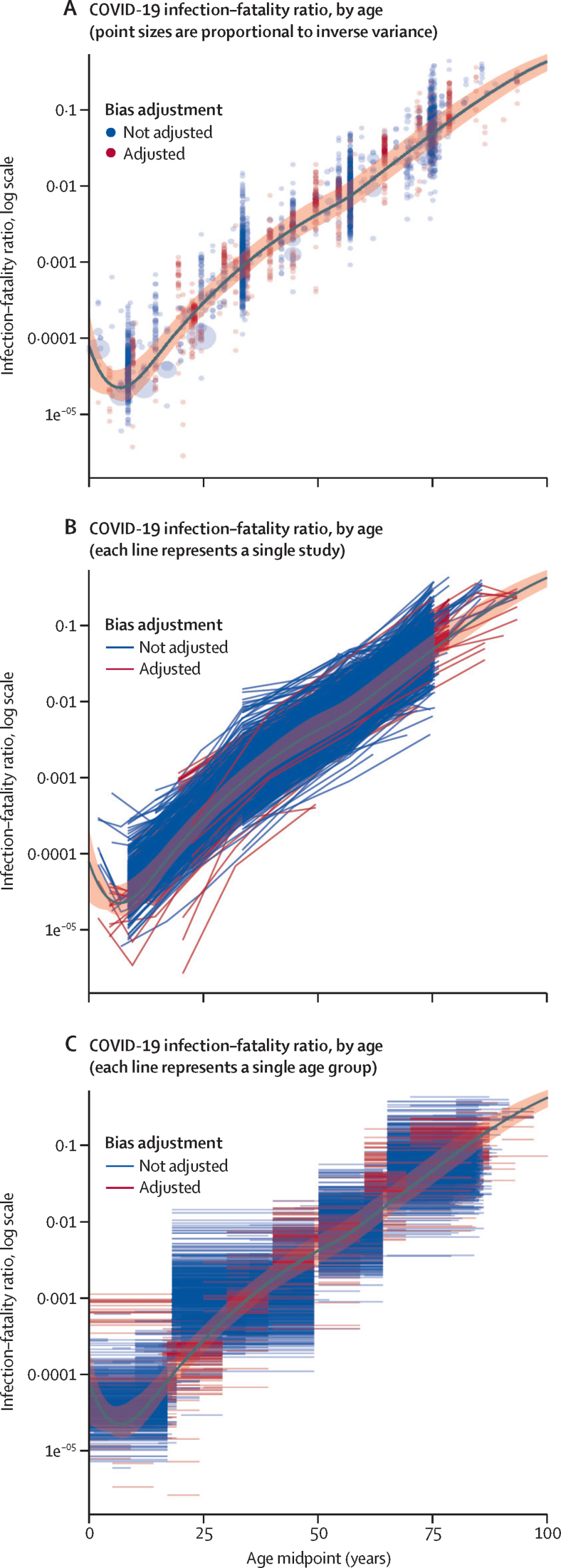
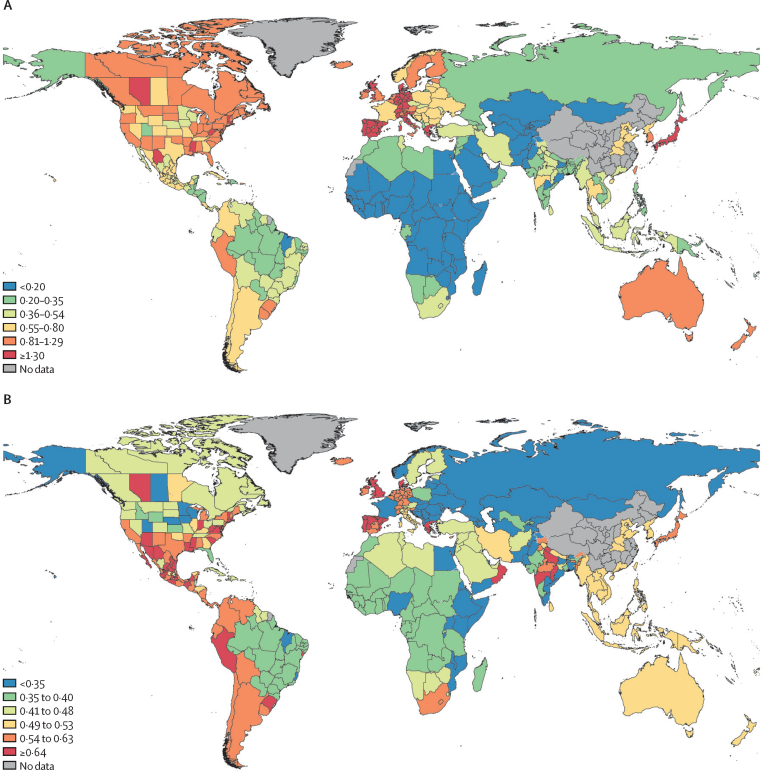
Findings: We report IFR estimates for April 15, 2020, to January 1, 2021, the period before the introduction of vaccines and widespread evolution of variants. We found substantial heterogeneity in the IFR by age, location, and time. Age-specific IFR estimates form a J shape, with the lowest IFR occurring at age 7 years (0·0023%, 95% uncertainty interval [UI] 0·0015-0·0039) and increasing exponentially through ages 30 years (0·0573%, 0·0418-0·0870), 60 years (1·0035%, 0·7002-1·5727), and 90 years (20·3292%, 14·6888-28·9754). The countries with the highest IFR on July 15, 2020, were Portugal (2·085%, 0·946-4·395), Monaco (1·778%, 1·265-2·915), Japan (1·750%, 1·302-2·690), Spain (1·710%, 0·991-2·718), and Greece (1·637%, 1·155-2·678). All-age IFR varied by a factor of more than 30 among 190 countries and territories. After age standardisation, the countries with the highest IFR on July 15, 2020, were Peru (0·911%, 0·636-1·538), Portugal (0·850%, 0·386-1·793), Oman (0·762%, 0·381-1·399), Spain (0·751%, 0·435-1·193), and Mexico (0·717%, 0·426-1·404). Subnational locations with high IFRs also included hotspots in the UK and southern and eastern states of the USA. Sub-Saharan African countries and Asian countries generally had the lowest all-age and age-standardised IFRs. Population age structure accounted for 74% of logit-scale variation in IFRs estimated for 39 in-sample countries on July 15, 2020. A post-hoc analysis showed that high rates of transmission in the care home population might account for higher IFRs in some locations. Among all countries and territories, we found that the median IFR decreased from 0·466% (interquartile range 0·223-0·840) to 0·314% (0·143-0·551) between April 15, 2020, and Jan 1, 2021.
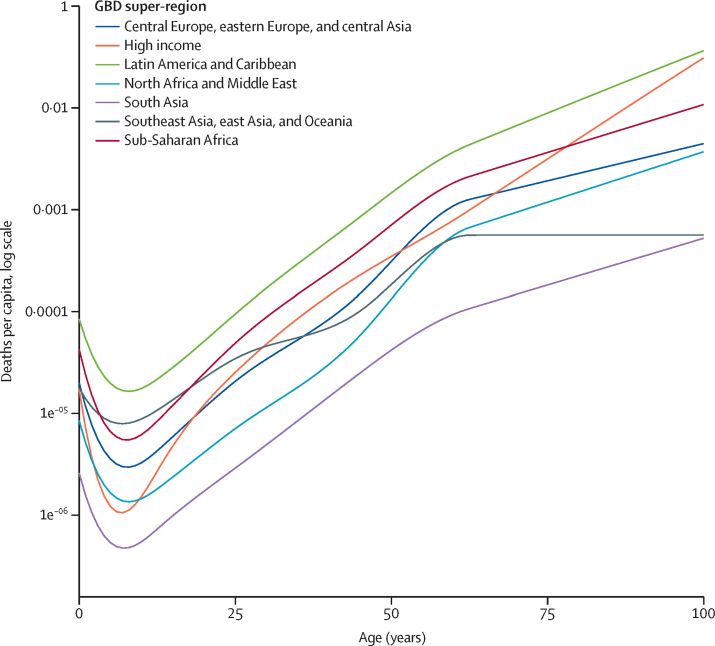
Interpretation: Estimating the IFR for global populations helps to identify relative vulnerabilities to COVID-19. Information about how IFR varies by age, time, and location informs clinical practice and non-pharmaceutical interventions like physical distancing measures, and underpins vaccine risk stratification. IFR and mortality risk form a J shape with respect to age, which previous research, such as that by Glynn and Moss in 2020, has identified to be a common pattern among infectious diseases. Understanding the experience of a population with COVID-19 mortality requires consideration for local factors; IFRs varied by a factor of more than 30 among 190 countries and territories in this analysis. In particular, the presence of elevated age-standardised IFRs in countries with well resourced health-care systems indicates that factors beyond health-care capacity are important. Potential extenuating circumstances include outbreaks among care home residents, variable burdens of severe cases, and the population prevalence of comorbid conditions that increase the severity of COVID-19 disease. During the pre-vaccine period, the estimated 33% decrease in median IFR over 8 months suggests that treatment for COVID-19 has improved over time. Estimating IFR for the pre-vaccine era provides an important baseline for describing the progression of COVID-19 mortality patterns.
Funding: Bill & Melinda Gates Foundation, J Stanton, T Gillespie, and J and E Nordstrom.
Copyright © 2022 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY-NC-ND 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests CA reports support for the present manuscript from the Benificus Foundation as funding support for the collection of data on state-level social-distancing policies in the USA. XD reports support for the present manuscript from the University of Washington through their employment at the Institute for Health Metrics and Evaluation. ADF reports stock or stock options in Agathos for technical advising, and other financial or non-financial interest from Janssen, SwissRe, Merck for Mothers, and Sanofi, for technical advising on simulation modelling, all outside the submitted work. NF reports receiving funding for work from WHO as a consultant from June, 2019, to September, 2019, and Gates Ventures since June, 2020, all outside the submitted work. SN reports support for the present manuscript from the Ministry of Education, Culture, Sports, Science and Technology of Japan as a grant. DMP report support for the present manuscript from the Bill & Melinda Gates Foundation. All other authors declare no competing interests.
Figures

Comment in
-
COVID-19 and microbiome diversity in sub-Saharan Africa.Lancet. 2022 Aug 6;400(10350):429. doi: 10.1016/S0140-6736(22)01333-2. Lancet. 2022. PMID: 35934003 Free PMC article. No abstract available.
References
-
- National Institutes of Health Overview of COVID-19. COVID-19 treatment guidelines. 2021. https://www.covid19treatmentguidelines.nih.gov/overview/ - PubMed
-
- Centers for Disease Control and Prevention How CDC is making COVID-19 vaccine recommendations. May 14, 2021. https://www.cdc.gov/coronavirus/2019-ncov/vaccines/recommendations-proce...
-
- Toner E, Barnill A, Krubiner C, et al. Johns Hopkins Center for Health Security; Baltimore: 2020. Interim framework for COVID-19 vaccine allocation and distribution in the United States.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
