

Should COVID-19 symptoms be used to cohort patients in the emergency department? A retrospective analysis
- PMID: 35220142
- PMCID: PMC8818126
- DOI: 10.1016/j.ajem.2022.01.070
Should COVID-19 symptoms be used to cohort patients in the emergency department? A retrospective analysis
Abstract
Objective: To determine how cohorting patients based on presenting complaints affects risk of nosocomial infection in crowded Emergency Departments (EDs) under conditions of high and low prevalence of COVID-19.
Methods: This was a retrospective analysis of presenting complaints and PCR tests collected during the COVID-19 epidemic from 4 EDs from a large hospital system in Bronx County, NY, from May 1, 2020 to April 30, 2021. Sensitivity, specificity, positive and negative predictive value (PPV, NPV) were calculated for a symptom screen based on the CDC list of COVID-19 symptoms: fever/chills, shortness of breath/dyspnea, cough, muscle or body ache, fatigue, headache, loss of taste or smell, sore throat, nasal congestion/runny nose, nausea, vomiting, and diarrhea. PPV was calculated for varying values of prevalence.
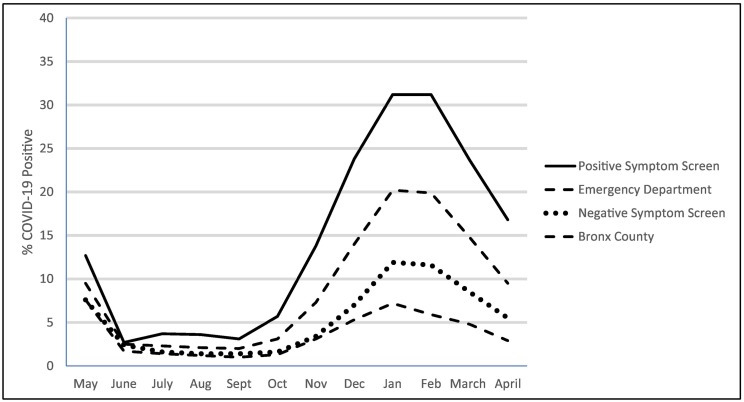
Results: There were 80,078 visits with PCR tests. The sensitivity of the symptom screen was 64.7% (95% CI: 63.6, 65.8), specificity 65.4% (65.1, 65.8). PPV was 16.8% (16.5, 17.0) and NPV was 94.5% (94.4, 94.7) when the observed prevalence of COVID-19 in the ED over the year was 9.7%. The PPV of fever/chills, cough, body and muscle aches and nasal congestion/runny nose were each approximately 25% across the year, while diarrhea, nausea, vomiting and headache were less predictive, (PPV 4.7%-9.6%) The combinations of fever/chills, cough, muscle/body aches, and shortness of breath had PPVs of 40-50%. The PPV of the screen varied from 3.7% (3.6, 3.8) at 2% prevalence of COVID-19 to 44.3% (44.0, 44.7) at 30% prevalence.
Conclusion: The proportion of patients with a chief complaint of COVID-19 symptoms and confirmed COVID-19 infection was exceeded by the proportion without actual infection. This was true when prevalence in the ED was as high as 30%. Cohorting of patients based on the CDC's list of COVID-19 symptoms will expose many patients who do not have COVID-19 to risk of nosocomially acquired COVID-19. EDs should not use the CDC list of COVID-19 symptoms as the only strategy to minimize exposure.
Keywords: COVID-19 testing; Emergency service, hospital; Predictive value of tests; Sensitivity and specificity.
Copyright © 2022 Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of Competing Interest There are no competing interests.
Figures
References
-
- Chu D.K., Akl E.A., Duda S., Solo K., Yaacoub S., Schünemann H.J., et al. Physical distancing, face masks, and eye protection to prevent person-to-person transmission of SARS-CoV-2 and COVID-19: a systematic review and meta-analysis. Lancet. 2020;395:1973–1987. doi: 10.1016/S0140-6736(20)31142-9. - DOI - PMC - PubMed
-
- Centers for Disease Control Guideline for isolation precautions: Preventing transmission of infectious agents in healthcare settings. 2007. https://www.cdc.gov/infectioncontrol/guidelines/isolation/prevention.html [accessed 11 November 2021] - PMC - PubMed
-
- Centers for Disease Control Symptoms of COVID-19. 2021. https://www.cdc.gov/coronavirus/2019-ncov/symptoms-testing/symptoms.html [accessed 1 November 2021]
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
