

Effects of Combing Group Executive Functioning and Online Parent Training on School-Aged Children With ADHD: A Randomized Controlled Trial
- PMID: 35223713
- PMCID: PMC8874140
- DOI: 10.3389/fped.2021.813305
Effects of Combing Group Executive Functioning and Online Parent Training on School-Aged Children With ADHD: A Randomized Controlled Trial
Abstract
Objective: The acceptance of drug treatment for younger children with attention-deficit/hyperactivity disorder (ADHD) in China remains low. Here, we explored the clinical benefits of a non-pharmaceutical intervention method combining a group and executive function training and an online parent training program, termed group executive functioning and online parent training (GEF-OPT), for school-aged students with ADHD through a randomized controlled trial.
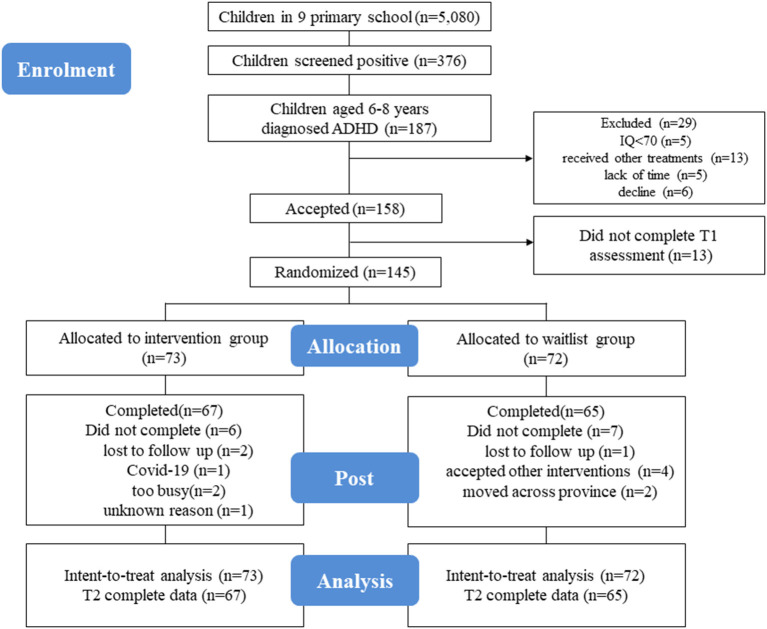
Method: A total of 145 children (aged 6-8 years) were formally registered and randomized to the intervention group (n = 73) and waitlist group (n = 72). The enrolled children received eight sessions of GEF-OPT treatment, which consists of a hospital-based children executive function (EF) training program and an online parent training program. Treatment outcome was assessed by a parent/teacher report questionnaire and neurophysiological experiment.
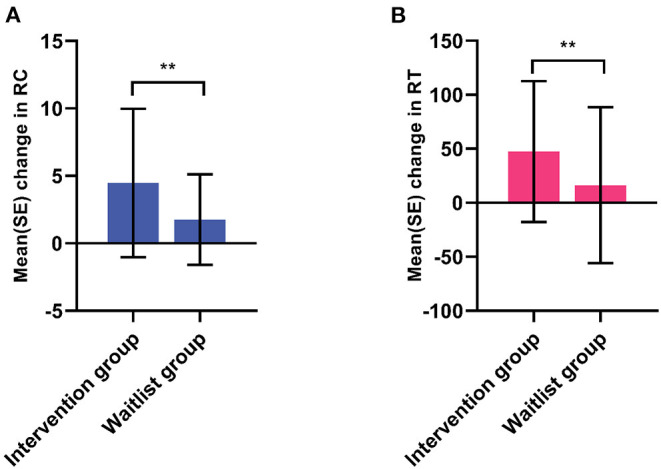
Results: After eight sessions of intervention, children in the intervention group showed a significant improvement in inattentive symptom compared to the waitlist group (14.70 ± 4.35 vs. 16.03 ± 2.93; p = 0.024), but an insignificant difference in hyperactive-impulsivity (9.85 ± 5.30 vs. 10.69 ± 5.10; p = 0.913). Comorbid oppositional defiant disorder was significantly reduced in the intervention group (7.03 ± 4.39 vs. 8.53 ± 4.41; p = 0.035). Children in the intervention group had greater reduction in the scores of behavioral regulation index (inhibition, emotional control) and metacognition index (working memory, planning/organization, monitoring) in executive function than those in the waitlist group (p < 0.05). Significant effects were also found in learning problem of Weiss Functional Impairment Scale-Parent form and parental distress between two groups at post-treatment (p < 0.05). In line with this, the result of go/no-go task showed significant improvements in accuracy change (4.45 ± 5.50% vs. 1.76 ± 3.35%; p = 0.001) and reaction time change (47.45 ± 62.25 s vs. 16.19 ± 72.22 s; p = 0.007) in the intervention group compared with the waitlist group.
Conclusion: We conclude that participants in the GEF-OPT program improved outcomes for inattentive symptom, executive function, learning problems, and parental distress. GEF-OPT is a promising non-pharmaceutical therapeutic option for younger children.
Trial registration: ChiCTR2100052803.
Keywords: ADHD; executive function; non-pharmacological treatment; online intervention; parent training.
Copyright © 2022 Chu, Zhu, Ma, Pan, Shen, Wu, Wang and Yu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. The handling editor FL declared a shared parent affiliation with the authors at the time of the review.
Figures
Similar articles
-
Effect of an Ecological Executive Skill Training Program for School-aged Children with Attention Deficit Hyperactivity Disorder: A Randomized Controlled Clinical Trial.Chin Med J (Engl). 2017 Jul 5;130(13):1513-1520. doi: 10.4103/0366-6999.208236. Chin Med J (Engl). 2017. PMID: 28639564 Free PMC article. Clinical Trial.
-
A Digital Cognitive-Physical Intervention for Attention-Deficit/Hyperactivity Disorder: Randomized Controlled Trial.J Med Internet Res. 2024 May 10;26:e55569. doi: 10.2196/55569. J Med Internet Res. 2024. PMID: 38728075 Free PMC article. Clinical Trial.
-
Effectiveness of Social Virtual Reality Training in Enhancing Social Interaction Skills in Children With Attention-Deficit/Hyperactivity Disorder: Protocol for a Three-Arm Pilot Randomized Controlled Trial.JMIR Res Protoc. 2023 Sep 18;12:e48208. doi: 10.2196/48208. JMIR Res Protoc. 2023. PMID: 37721790 Free PMC article.
-
Social skills training for attention deficit hyperactivity disorder (ADHD) in children aged 5 to 18 years.Cochrane Database Syst Rev. 2019 Jun 21;6(6):CD008223. doi: 10.1002/14651858.CD008223.pub3. Cochrane Database Syst Rev. 2019. PMID: 31222721 Free PMC article.
-
Which Factor Is More Relevant to the Effectiveness of the Cognitive Intervention? A Meta-Analysis of Randomized Controlled Trials of Cognitive Training on Symptoms and Executive Function Behaviors of Children With Attention Deficit Hyperactivity Disorder.Front Psychol. 2022 Jan 13;12:810298. doi: 10.3389/fpsyg.2021.810298. eCollection 2021. Front Psychol. 2022. PMID: 35095697 Free PMC article. Review.
Cited by
-
Systematic Review of Executive Function Stimulation Methods in the ADHD Population.J Clin Med. 2024 Jul 19;13(14):4208. doi: 10.3390/jcm13144208. J Clin Med. 2024. PMID: 39064248 Free PMC article. Review.
-
Evolving role of the internet in China as a medium for promoting psychological well-being and mental health: a scoping review.Lancet Reg Health West Pac. 2025 Mar 19;56:101515. doi: 10.1016/j.lanwpc.2025.101515. eCollection 2025 Mar. Lancet Reg Health West Pac. 2025. PMID: 40226776 Free PMC article. Review.
-
A naturalistic virtual reality task reveals difficulties in time-based prospective memory and strategic time-monitoring in children with ADHD.Sci Rep. 2025 Jul 9;15(1):24722. doi: 10.1038/s41598-025-08944-w. Sci Rep. 2025. PMID: 40634396 Free PMC article.
-
Online Parenting Programs for Children's Behavioral and Emotional Problems: a Network Meta-Analysis.Prev Sci. 2025 May;26(4):592-609. doi: 10.1007/s11121-024-01735-1. Epub 2024 Oct 13. Prev Sci. 2025. PMID: 39397230 Free PMC article.
-
Behavioural interventions targeting the prevention and treatment of young children's mental health problems in low- and middle-income countries: a scoping review.J Glob Health. 2025 Jan 24;15:04018. doi: 10.7189/jogh.15.04018. J Glob Health. 2025. PMID: 39849969 Free PMC article.
References
-
- Catala-Lopez F, Hutton B, Nunez-Beltran A, Page MJ, Ridao M, Macias Saint-Gerons D, et al. . The pharmacological and non-pharmacological treatment of attention deficit hyperactivity disorder in children and adolescents: a systematic review with network meta-analyses of randomised trials. PLoS ONE. (2017) 12:e0180355. 10.1371/journal.pone.0180355 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources