

Developing and Validating Nomogram to Predict Severe Postpartum Hemorrhage in Women With Placenta Previa Undergoing Cesarean Delivery: A Multicenter Retrospective Case-Control Study
- PMID: 35223881
- PMCID: PMC8873861
- DOI: 10.3389/fmed.2021.789529
Developing and Validating Nomogram to Predict Severe Postpartum Hemorrhage in Women With Placenta Previa Undergoing Cesarean Delivery: A Multicenter Retrospective Case-Control Study
Abstract
Objective: Developing and validating nomogram to predict severe postpartum hemorrhage (SPPH) in women with placenta previa (PP) undergoing cesarean delivery.
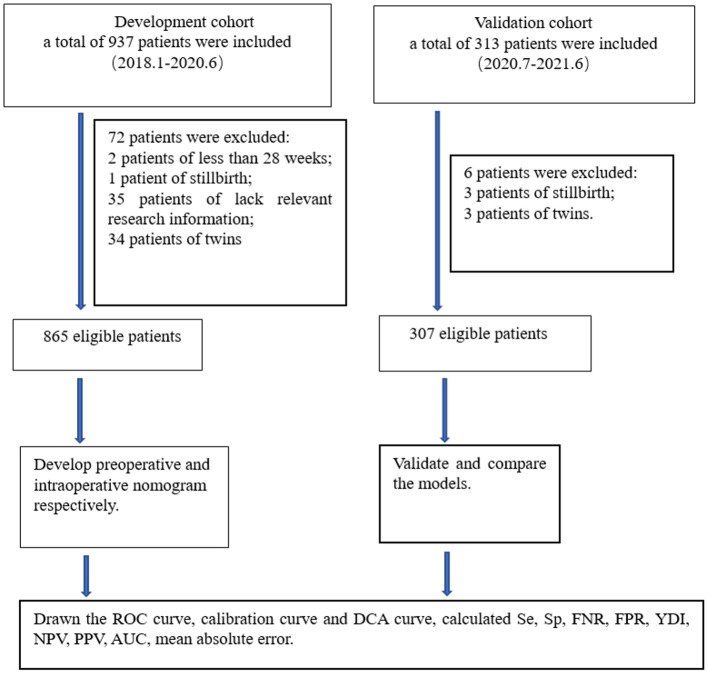
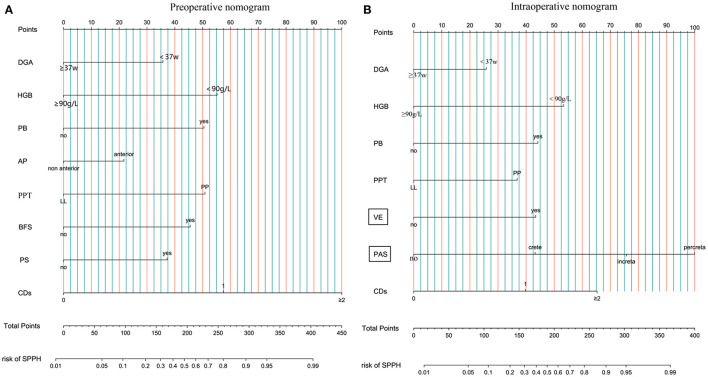
Methods: We conducted a multicenter retrospective case-control study in five hospitals. In this study, 865 patients from January, 2018 to June, 2020 were enrolled in the development cohort, and 307 patients from July, 2020 to June, 2021 were enrolled in the validation cohort. Independent risk factors for SPPH were obtained by using the multivariate logistic regression, and preoperative nomogram and intraoperative nomogram were developed, respectively. We compared the discrimination, calibration, and net benefit of the two nomograms in the development cohort and validation cohort. Then, we tested whether the intraoperative nomogram could be used before operation.
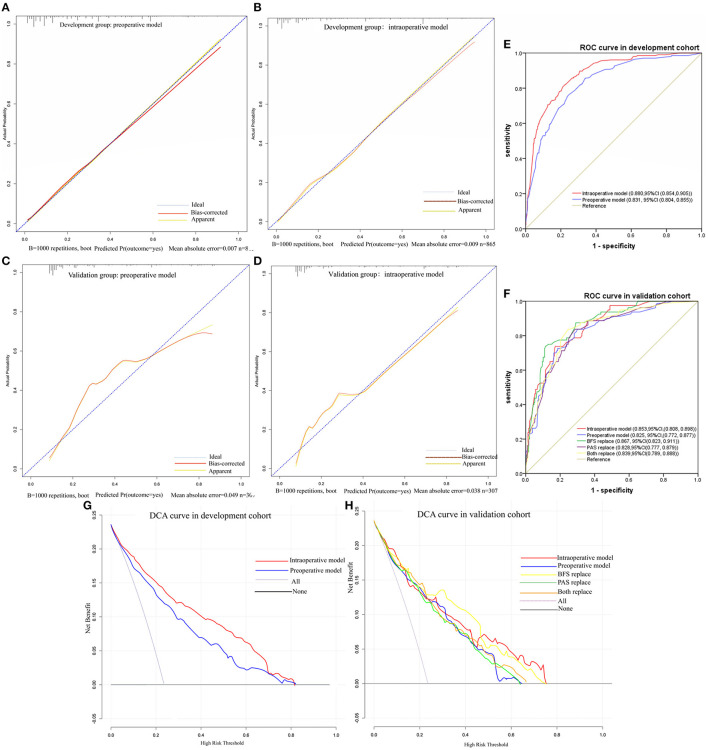
Results: There were 204 patients (23.58%) in development cohort and 80 patients (26.06%) in validation cohort experienced SPPH. In development cohort, the areas under the receiver operating characteristic (ROC) curve (AUC) of the preoperative nomogram and intraoperative nomogram were 0.831 (95% CI, 0.804, 0.855) and 0.880 (95% CI, 0.854, 0.905), respectively. In validation cohort, the AUC of the preoperative nomogram and intraoperative nomogram were 0.825 (95% CI, 0.772, 0.877) and 0.853 (95% CI, 0.808, 0.898), respectively. In the validation cohort, the AUC was 0.839 (95% CI, 0.789, 0.888) when the intraoperative nomogram was used before operation.
Conclusion: We developed the preoperative nomogram and intraoperative nomogram to predict the risk of SPPH in women with PP undergoing cesarean delivery. By comparing the discrimination, calibration, and net benefit of the two nomograms in the development cohort and validation cohort, we think that the intraoperative nomogram performed better. Moreover, application of the intraoperative nomogram before operation can still achieve good prediction effect, which can be improved if the severity of placenta accreta spectrum (PAS) can be accurately distinguished preoperatively. We expect to conduct further prospective external validation studies on the intraoperative nomogram to evaluate its application value.
Keywords: multivariate logistic regression; nomogram; placenta previa; prediction model; severe postpartum hemorrhage.
Copyright © 2022 Dang, Zhang, Bao, Xu, Du, Wang, Liu, Deng, Chen, Zeng, Feng and Liu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Nomogram based on clinical characteristics and ultrasound indicators for predicting severe postpartum hemorrhage in patients with anterior placenta previa combined with previous cesarean section: a retrospective case-control study.BMC Pregnancy Childbirth. 2024 Aug 31;24(1):572. doi: 10.1186/s12884-024-06706-6. BMC Pregnancy Childbirth. 2024. PMID: 39217290 Free PMC article.
-
Magnetic Resonance Imaging-Based Radiomics Nomogram to Predict Intraoperative Hemorrhage of Placenta Previa.Am J Perinatol. 2024 May;41(S 01):e2174-e2183. doi: 10.1055/a-2099-3809. Epub 2023 May 24. Am J Perinatol. 2024. PMID: 37225126
-
Systematic external evaluation of four preoperative risk prediction models for severe postpartum hemorrhage in patients with placenta previa: A multicenter retrospective study.J Gynecol Obstet Hum Reprod. 2022 Apr;51(4):102333. doi: 10.1016/j.jogoh.2022.102333. Epub 2022 Feb 10. J Gynecol Obstet Hum Reprod. 2022. PMID: 35151929
-
Development and validation of a nomogram for predicting placenta accreta spectrum in pregnancies with one previous cesarean delivery.Int J Gynaecol Obstet. 2024 Nov;167(2):685-694. doi: 10.1002/ijgo.15702. Epub 2024 Jun 4. Int J Gynaecol Obstet. 2024. PMID: 38832362
-
Development of a nomogram for severe influenza in previously healthy children: a retrospective cohort study.J Int Med Res. 2023 Feb;51(2):3000605231153768. doi: 10.1177/03000605231153768. J Int Med Res. 2023. PMID: 36802862 Free PMC article. Review.
Cited by
-
Risk factors for postpartum hemorrhage in critically ill pregnant women with placenta previa and construction of a dynamic nomogram model.Am J Transl Res. 2025 Mar 15;17(3):1834-1847. doi: 10.62347/QKFG5933. eCollection 2025. Am J Transl Res. 2025. PMID: 40226028 Free PMC article.
-
Association of Placenta Previa With Severe Maternal Morbidity Among Patients With Placenta Accreta Spectrum Disorder.JAMA Netw Open. 2022 Aug 1;5(8):e2228002. doi: 10.1001/jamanetworkopen.2022.28002. JAMA Netw Open. 2022. PMID: 35994286 Free PMC article.
References
-
- Centers for Disease Control and Prevention . Pregnancy Mortality Surveillance System. Available online at: http://www.cdc.gov/reproductivehealth/maternalinfanthealth/pmss.html (accessed July 21, 2019).
LinkOut - more resources
Full Text Sources
Miscellaneous