

Long-Term Persisting SARS-CoV-2 RNA and Pathological Findings: Lessons Learnt From a Series of 35 COVID-19 Autopsies
- PMID: 35223894
- PMCID: PMC8865372
- DOI: 10.3389/fmed.2022.778489
Long-Term Persisting SARS-CoV-2 RNA and Pathological Findings: Lessons Learnt From a Series of 35 COVID-19 Autopsies
Abstract
Background: Long-term sequelae of coronavirus disease 2019 (COVID-19), including the interaction between persisting viral-RNA and specific tissue involvement, pose a challenging issue. In this study, we addressed the chronological correlation (after first clinical diagnosis and postmortem) between severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) RNA and organ involvement.
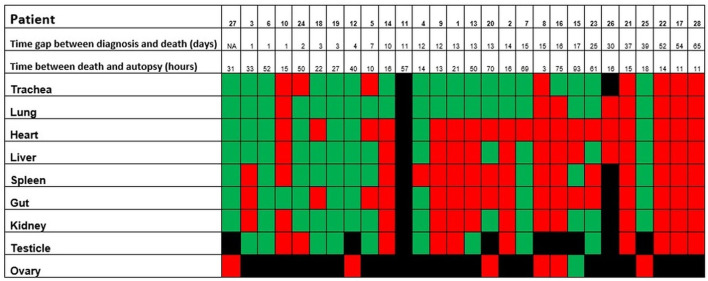
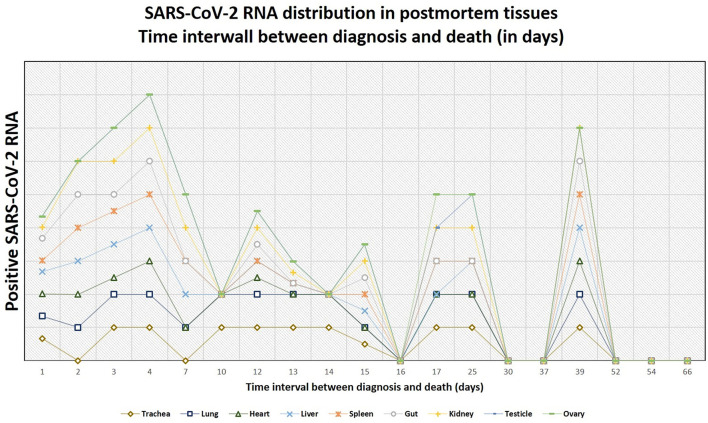
Methods: The presence of postmortem SARS-CoV-2 RNA from 35 complete COVID-19 autopsies was correlated with the time interval between the first diagnosis of COVID-19 and death and with its relationship to morphologic findings.
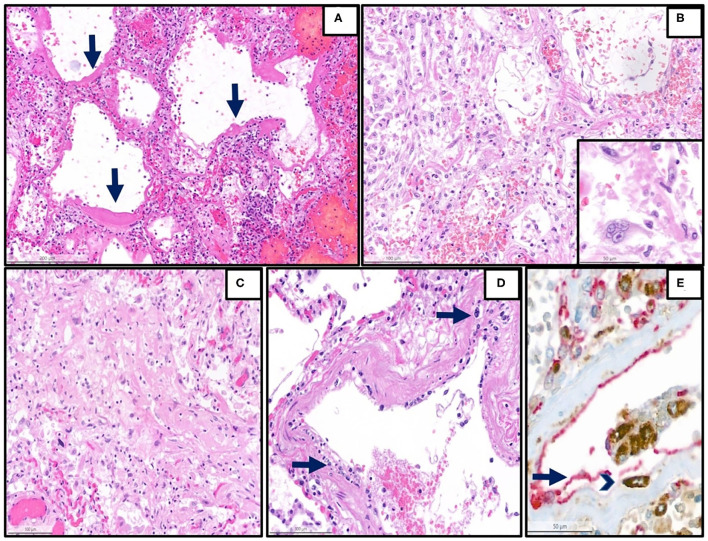
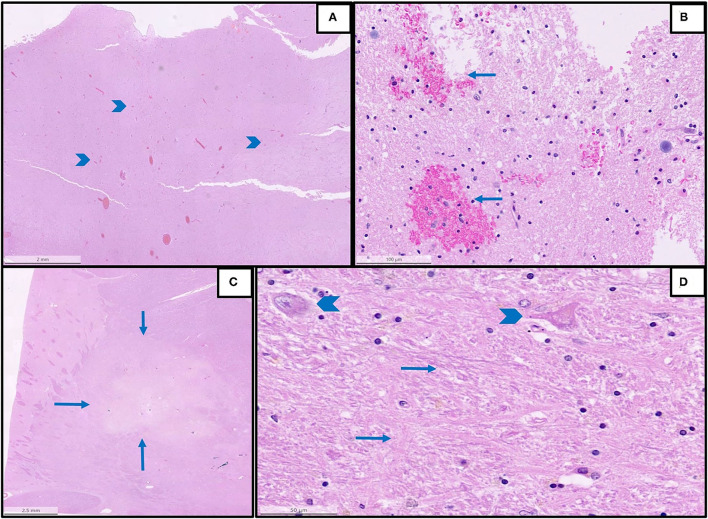
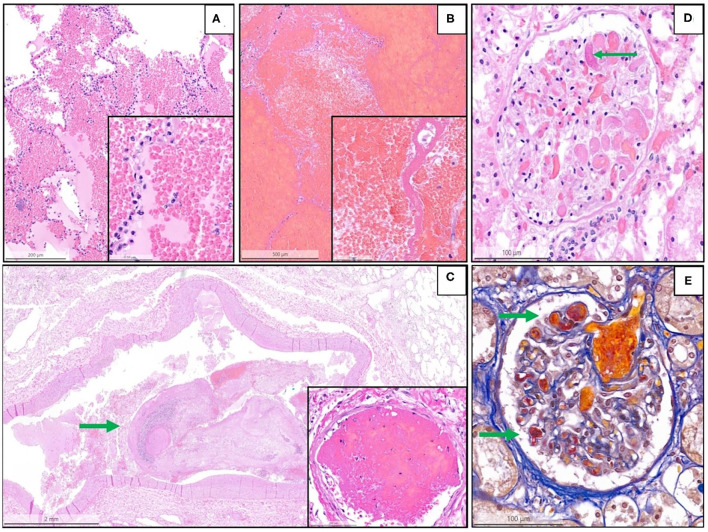
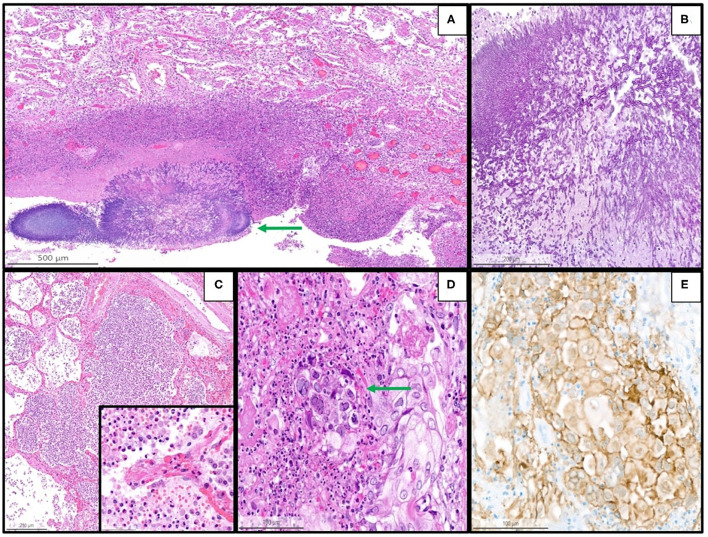
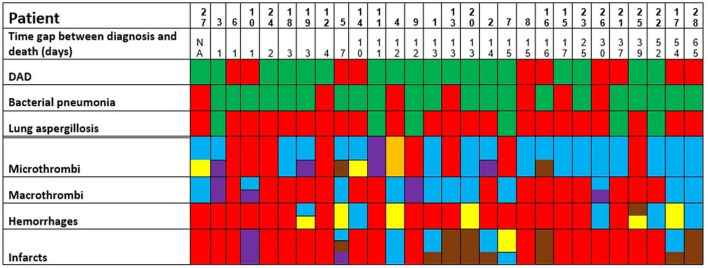
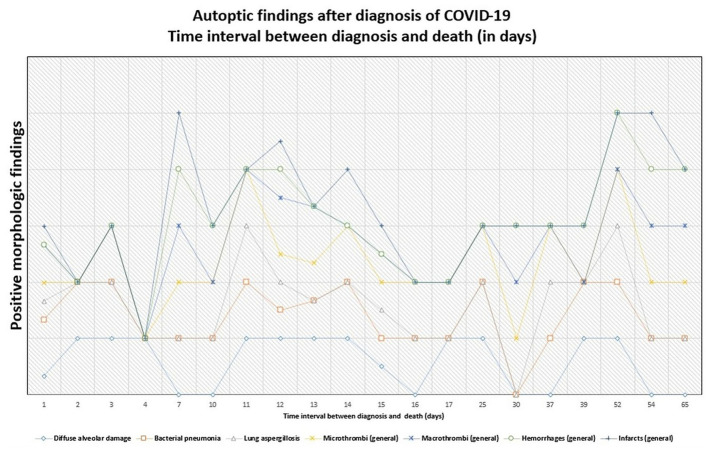
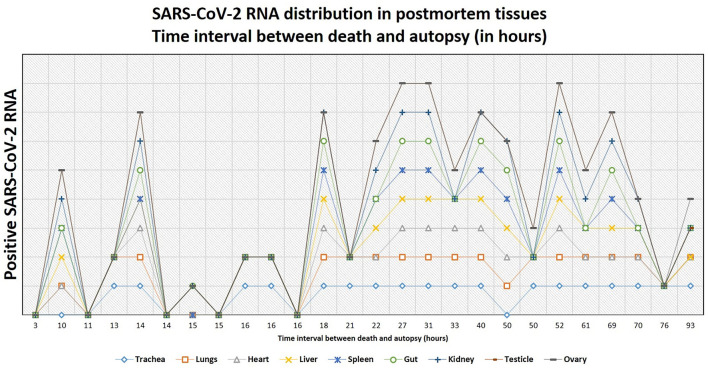
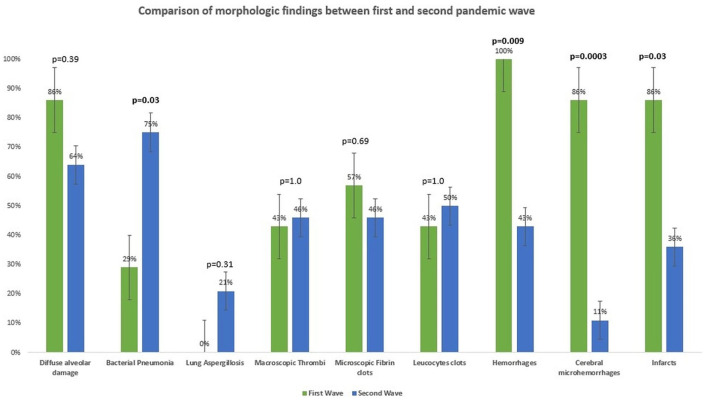
Results: Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) RNA can be evident up to 40 days after the first diagnosis and can persist to 94 hours after death. Postmortem SARS-CoV-2 RNA was mostly positive in lungs (70%) and trachea (69%), but all investigated organs were positive with variable frequency. Late-stage tissue damage was evident up to 65 days after initial diagnosis in several organs. Positivity for SARS-CoV-2 RNA in pulmonary swabs correlated with diffuse alveolar damage (p = 0.0009). No correlation between positive swabs and other morphologic findings was present. Cerebral (p = 0.0003) and systemic hemorrhages (p = 0.009), cardiac thrombi (p = 0.04), and ischemic events (p = 0.03) were more frequent in the first wave, whereas bacterial pneumonia (p = 0.03) was more prevalent in the second wave. No differences in biometric data, clinical comorbidities, and other autopsy findings were found.
Conclusions: Our data provide evidence not only of long-term postmortem persisting SARS-CoV-2 RNA but also of tissue damage several weeks after the first diagnosis of SARS-CoV-2 infection. Additional conditions, such as concomitant bacterial pulmonary superinfection, lung aspergillosis, thromboembolic phenomena, and hemorrhages can further worsen tissue damage.
Keywords: COVID-19; SARS-CoV-2 RNA PCR; autopsy; histopathology; long-COVID; postmortal swabs; pulmonary superinfections.
Copyright © 2022 Maccio, Zinkernagel, Schuepbach, Probst-Mueller, Frontzek, Brugger, Hofmaenner, Moch and Varga.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
COVID-19 Autopsies, Oklahoma, USA.Am J Clin Pathol. 2020 May 5;153(6):725-733. doi: 10.1093/ajcp/aqaa062. Am J Clin Pathol. 2020. PMID: 32275742 Free PMC article.
-
Autopsy-Based Pulmonary and Vascular Pathology: Pulmonary Endotheliitis and Multi-Organ Involvement in COVID-19 Associated Deaths.Respiration. 2022;101(2):155-165. doi: 10.1159/000518914. Epub 2021 Sep 15. Respiration. 2022. PMID: 34525475 Free PMC article.
-
Dying with SARS-CoV-2 infection-an autopsy study of the first consecutive 80 cases in Hamburg, Germany.Int J Legal Med. 2020 Jul;134(4):1275-1284. doi: 10.1007/s00414-020-02317-w. Epub 2020 Jun 4. Int J Legal Med. 2020. PMID: 32500199 Free PMC article.
-
COVID-19 in the Netherlands: lessons from a nationwide query of dutch autopsy, histology, and cytology pathological reports.Virchows Arch. 2024 Mar;484(3):429-439. doi: 10.1007/s00428-024-03771-2. Epub 2024 Feb 27. Virchows Arch. 2024. PMID: 38413389 Free PMC article. Review.
-
[SARS-CoV-2 and Microbiological Diagnostic Dynamics in COVID-19 Pandemic].Mikrobiyol Bul. 2020 Jul;54(3):497-509. doi: 10.5578/mb.69839. Mikrobiyol Bul. 2020. PMID: 32755524 Review. Turkish.
Cited by
-
Autonomic Nerve Involvement in Post-Acute Sequelae of SARS-CoV-2 Syndrome (PASC).J Clin Med. 2022 Dec 22;12(1):73. doi: 10.3390/jcm12010073. J Clin Med. 2022. PMID: 36614874 Free PMC article.
-
Effect of obesity on the acute response to SARS-CoV-2 infection and development of post-acute sequelae of COVID-19 (PASC) in nonhuman primates.bioRxiv [Preprint]. 2025 Feb 22:2025.02.18.638792. doi: 10.1101/2025.02.18.638792. bioRxiv. 2025. Update in: PLoS Pathog. 2025 Jul 24;21(7):e1012988. doi: 10.1371/journal.ppat.1012988. PMID: 40027795 Free PMC article. Updated. Preprint.
-
Effect of obesity on the acute response to SARS-CoV-2 infection and development of post-acute sequelae of COVID-19 (PASC) in nonhuman primates.PLoS Pathog. 2025 Jul 24;21(7):e1012988. doi: 10.1371/journal.ppat.1012988. eCollection 2025 Jul. PLoS Pathog. 2025. PMID: 40705709 Free PMC article.
-
Sequelae of COVID-19 among previously hospitalized patients up to 1 year after discharge: a systematic review and meta-analysis.Infection. 2022 Oct;50(5):1067-1109. doi: 10.1007/s15010-022-01862-3. Epub 2022 Jun 24. Infection. 2022. PMID: 35750943 Free PMC article.
-
Biofilms possibly harbor occult SARS-CoV-2 may explain lung cavity, re-positive and long-term positive results.Front Cell Infect Microbiol. 2022 Sep 28;12:971933. doi: 10.3389/fcimb.2022.971933. eCollection 2022. Front Cell Infect Microbiol. 2022. PMID: 36250053 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Miscellaneous