

Case report of the broad spectrum of late complications in an adult patient with univentricular physiology palliated by the Fontan circulation
- PMID: 35224438
- PMCID: PMC8867817
- DOI: 10.1093/ehjcr/ytac067
Case report of the broad spectrum of late complications in an adult patient with univentricular physiology palliated by the Fontan circulation
Abstract
Background: At the most severe end of the spectrum of congenital heart disease are patients with an univentricular physiology. They comprise a heterogeneous group of congenital heart malformations that have the common characteristic that the cardiac morphology is not equipped for sustaining a biventricular circulation.
Case summary: Here, we present a case of an adult patient after Fontan palliation, illustrative of the complex clinical course and the broad spectrum of complications that can be encountered during follow-up, highlighting the need for a multidisciplinary approach in the clinical care for these patients.
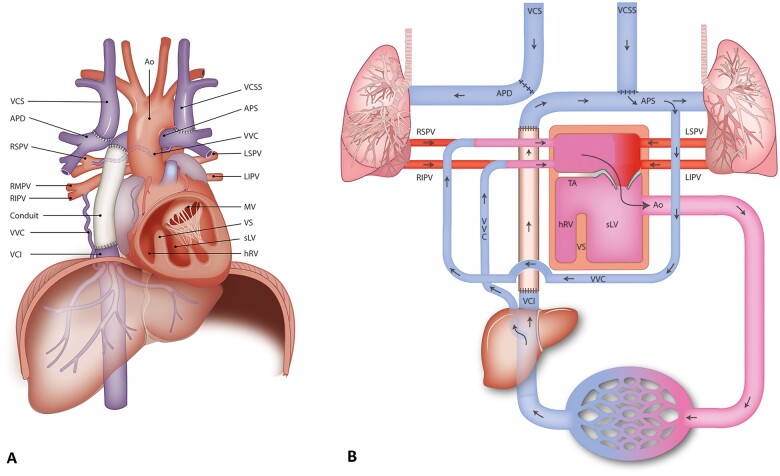
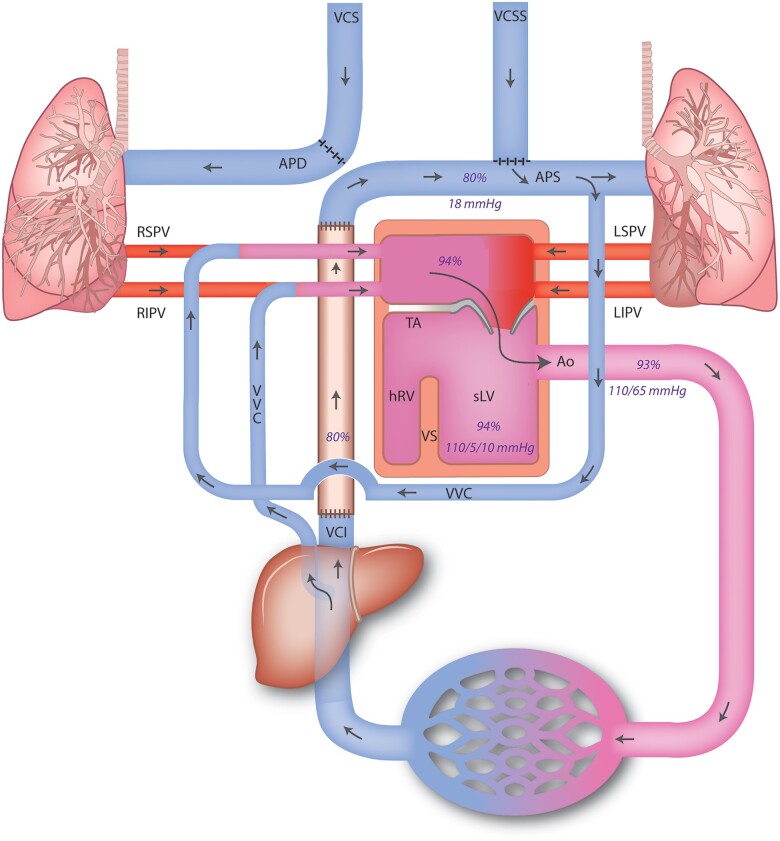
Discussion: During the surgical Fontan procedure, the inferior vena cava is connected to the pulmonary circulation, after prior connection of the superior vena cava to the pulmonary arterial circulation. The resulting cavopulmonary connection, thus lacking a subpulmonic ventricle, provides non-pulsatile passive flow of oxygen-poor blood from the systemic venous circulation into the lungs, and the functional monoventricle pumps the oxygen-rich pulmonary venous return blood into the aorta. With an operative mortality of <5% and current 30-year survival rates up to 85%, the adult population of patients with a Fontan circulation is growing. This increase in survival is, however, inevitably accompanied by long-term complications affecting multiple organ systems, resulting in decline in cardiovascular performance.
Conclusion: For optimal treatment, the evaluation in a multidisciplinary team is mandatory, using the specific expertise of the team members to timely detect and address late complications and to support quality of life.
Keywords: Case report; Congenital heart disease; Fontan circulation; Fontan failure; Fontan-related liver disease; Long-term complications; Univentricular heart.
© The Author(s) 2022. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures
References
-
- Baumgartner H, De Backer J, Babu-Narayan SV, Budts W, Chessa M, Diller G-P. et al. 2020 ESC Guidelines for the management of adult congenital heart disease: The Task Force for the management of adult congenital heart disease of the European Society of Cardiology (ESC). Eur Heart J 2020;41:4153–4154. - PubMed
-
- Rychik J, Atz AM, Celermajer DS, Deal BJ, Gatzoulis MA, Gewillig MH. et al. ; On behalf of the American Heart Association Council on Cardiovascular Disease in the Young and Council on Cardiovascular and Stroke Nursing. Evaluation and management of the child and adult with fontan circulation: a scientific statement from the American Heart Association. Circulation 2019;140:e234–e284. - PubMed
-
- van Melle JP, Wolff D, Horer J, Belli E, Meyns B, Padalino M. et al. Surgical options after Fontan failure. Heart 2016;102:1127–1133. - PubMed
-
- Schuuring MJ, Vis JC, van Dijk AP, van Melle JP, Vliegen HW, Pieper PG. et al. Impact of bosentan on exercise capacity in adults after the Fontan procedure: a randomized controlled trial. Eur J Heart Fail 2013;15:690–698. - PubMed
-
- Sumal AS, Kyriacou H, Mostafa A.. Tricuspid atresia: where are we now? J Card Surg 2020;35:1609–1617. - PubMed
Publication types
LinkOut - more resources
Full Text Sources