

Preoperative Neutrophil-BMI Ratio As a Promising New Marker for Predicting Tumor Outcomes in Colorectal Cancer
- PMID: 35225701
- PMCID: PMC8891895
- DOI: 10.1177/15330338211064077
Preoperative Neutrophil-BMI Ratio As a Promising New Marker for Predicting Tumor Outcomes in Colorectal Cancer
Abstract
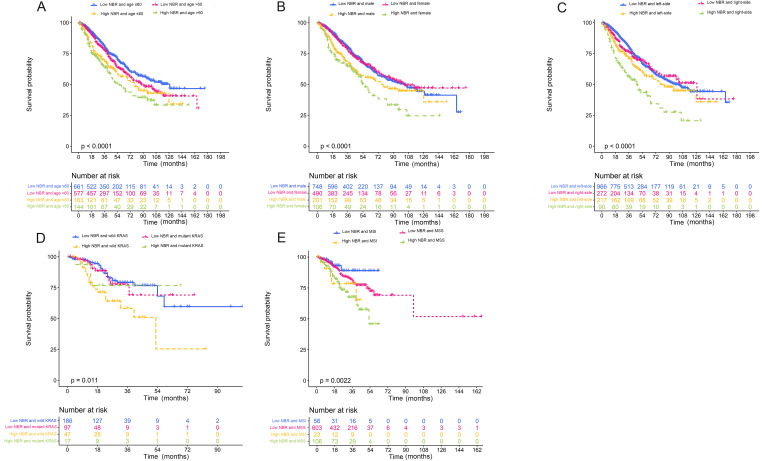
Background: Inflammation and nutritional status are highly associated with colorectal cancer (CRC) prognosis. This study aimed to evaluate the prognostic value of the preoperative neutrophil-BMI ratio (NBR) in patients with CRC. Methods: A retrospective analysis was performed on 2471 patients with CRC who underwent surgical resection between 2004 and 2019. Patients were divided into two groups based on the cutoff value for NBR. Cox regression and Kaplan-Meier curves were used to evaluate overall survival (OS). Results: High NBR was associated with female sex, low BMI, colon, right-sided CRC, poor differentiation, T3 to 4 stage, M1 to 2 stage, high carcinoembryonic antigen (CEA) level, III-IV stage, microsatellite instability (MSI), and no adjuvant chemotherapy (all P < .05). The high NBR group had a shorter OS than the low NBR group. Female and right sided patients with CRC and with high NBR had a worse prognosis. Univariate Cox regression suggested that NBR was significantly associated with poor prognosis. Multivariate analysis confirmed that age (P = .019,HR:1.012), differentiation (P = .001,HR:1.306), TNM stage (P < .001,HR:2.432), CEA (P = .014,HR:1.001), and NBR (P < .001, HR: 3.309) were independent poor prognostic factors for OS. Subgroup univariate analysis indicated that female patients with high NBR had a worse prognosis. A nomogram composed of TNM stage, CEA, and NBR was developed, and internal validation was based on female patients with CRC. The nomogram provided good discrimination for both the training and validation sets, with area under the curve values of 0.79 and 0.769, respectively. Conclusions: High preoperative levels of NBR are indicators of poor prognosis in patients with CRC.
Keywords: colorectal cancer; neutrophil-BMI ratio; nomogram; prognostic indicator; survival.
Conflict of interest statement
Figures




References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
