

A Smartphone-Based Model of Care to Support Patients With Cardiac Disease Transitioning From Hospital to the Community (TeleClinical Care): Pilot Randomized Controlled Trial
- PMID: 35225819
- PMCID: PMC8922139
- DOI: 10.2196/32554
A Smartphone-Based Model of Care to Support Patients With Cardiac Disease Transitioning From Hospital to the Community (TeleClinical Care): Pilot Randomized Controlled Trial
Abstract
Background: Patients hospitalized with acute coronary syndrome (ACS) or heart failure (HF) are frequently readmitted. This is the first randomized controlled trial of a mobile health intervention that combines telemonitoring and education for inpatients with ACS or HF to prevent readmission.
Objective: This study aims to investigate the feasibility, efficacy, and cost-effectiveness of a smartphone app-based model of care (TeleClinical Care [TCC]) in patients discharged after ACS or HF admission.
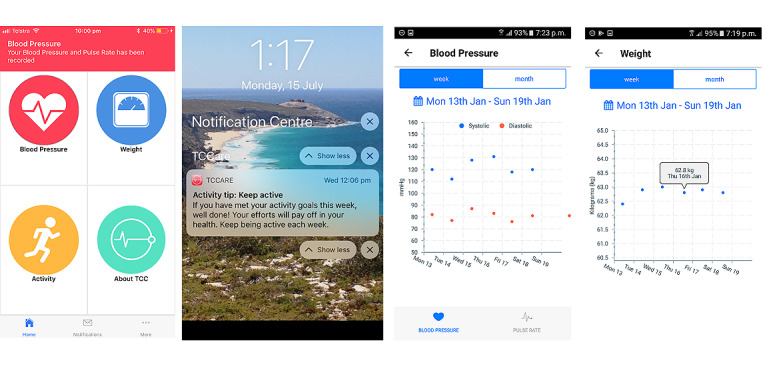
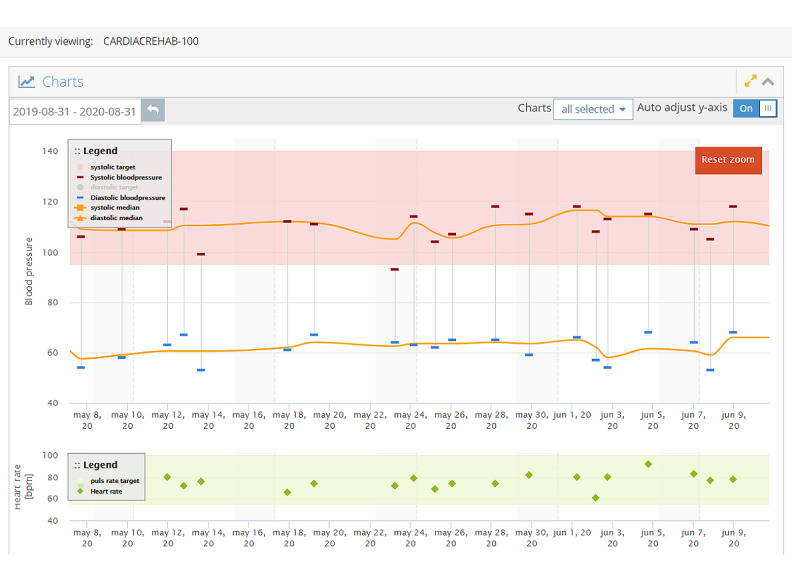
Methods: In this pilot, 2-center randomized controlled trial, TCC was applied at discharge along with usual care to intervention arm participants. Control arm participants received usual care alone. Inclusion criteria were current admission with ACS or HF, ownership of a compatible smartphone, age ≥18 years, and provision of informed consent. The primary end point was the incidence of unplanned 30-day readmissions. Secondary end points included all-cause readmissions, cardiac readmissions, cardiac rehabilitation completion, medication adherence, cost-effectiveness, and user satisfaction. Intervention arm participants received the app and Bluetooth-enabled devices for measuring weight, blood pressure, and physical activity daily plus usual care. The devices automatically transmitted recordings to the patients' smartphones and a central server. Thresholds for blood pressure, heart rate, and weight were determined by the treating cardiologists. Readings outside these thresholds were flagged to a monitoring team, who discussed salient abnormalities with the patients' usual care providers (cardiologists, general practitioners, or HF outreach nurses), who were responsible for further management. The app also provided educational push notifications. Participants were followed up after 6 months.
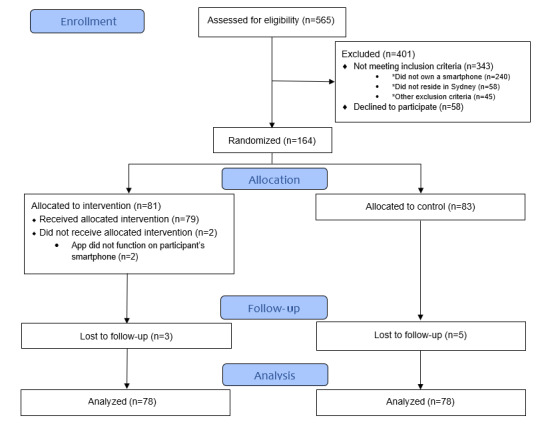
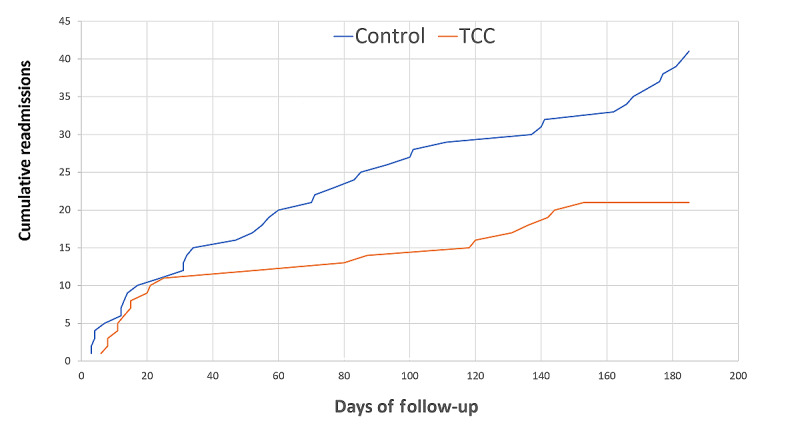
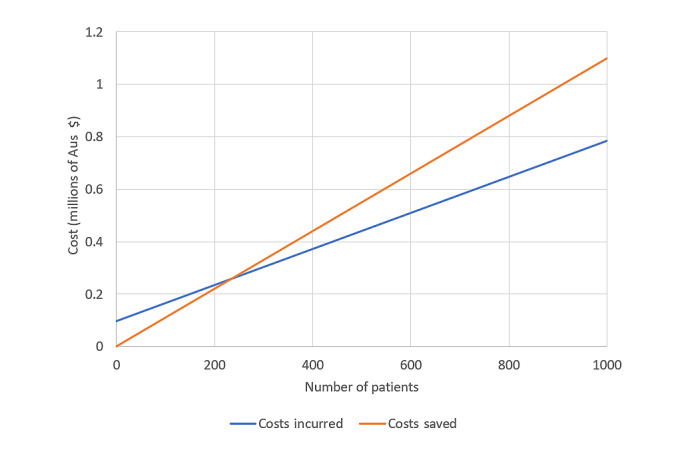
Results: Overall, 164 inpatients were randomized (TCC: 81/164, 49.4%; control: 83/164, 50.6%; mean age 61.5, SD 12.3 years; 130/164, 79.3% men; 128/164, 78% admitted with ACS). There were 11 unplanned 30-day readmissions in both groups (P=.97). Over a mean follow-up of 193 days, the intervention was associated with a significant reduction in unplanned hospital readmissions (21 in TCC vs 41 in the control arm; P=.02), including cardiac readmissions (11 in TCC vs 25 in the control arm; P=.03), and higher rates of cardiac rehabilitation completion (20/51, 39% vs 9/49, 18%; P=.03) and medication adherence (57/76, 75% vs 37/74, 50%; P=.002). The average usability rating for the app was 4.5/5. The intervention cost Aus $6028 (US $4342.26) per cardiac readmission saved. When modeled in a mainstream clinical setting, enrollment of 237 patients was projected to have the same expenditure compared with usual care, and enrollment of 500 patients was projected to save approximately Aus $100,000 (approximately US $70,000) annually.
Conclusions: TCC was feasible and safe for inpatients with either ACS or HF. The incidence of 30-day readmissions was similar; however, long-term benefits were demonstrated, including fewer readmissions over 6 months, improved medication adherence, and improved cardiac rehabilitation completion.
Trial registration: Australian New Zealand Clinical Trials Registry ACTRN12618001547235; https://www.anzctr.org.au/Trial/Registration/TrialReview.aspx?id=375945.
Keywords: digital health; heart failure; ischemic heart disease; mHealth; mobile phone; telemedicine.
©Praveen Indraratna, Uzzal Biswas, James McVeigh, Andrew Mamo, Joseph Magdy, Dominic Vickers, Elaine Watkins, Andreas Ziegl, Hueiming Liu, Nicholas Cholerton, Joan Li, Katie Holgate, Jennifer Fildes, Robyn Gallagher, Cate Ferry, Stephen Jan, Nancy Briggs, Guenter Schreier, Stephen J Redmond, Eugene Loh, Jennifer Yu, Nigel H Lovell, Sze-Yuan Ooi. Originally published in JMIR mHealth and uHealth (https://mhealth.jmir.org), 28.02.2022.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures

References
-
- Jayaraj JC, Davatyan K, Subramanian S, Priya J. Epidemiology of Myocardial Infarction. London, UK: Intech Open; 2018.
-
- Savarese G, Lund LH. Global public health burden of heart failure. Card Fail Rev. 2017 Apr;3(1):7–11. doi: 10.15420/cfr.2016:25:2. http://europepmc.org/abstract/MED/28785469 - DOI - PMC - PubMed
-
- Zou Z, Cini K, Dong B, Ma Y, Ma J, Burgner DP, Patton GC. Time trends in cardiovascular disease mortality across the BRICS: an age-period-cohort analysis of key nations with emerging economies using the global burden of disease study 2017. Circulation. 2020 Mar 10;141(10):790–9. doi: 10.1161/CIRCULATIONAHA.119.042864. - DOI - PubMed
-
- Lawson CA, Zaccardi F, Squire I, Ling S, Davies MJ, Lam CS, Mamas MA, Khunti K, Kadam UT. 20-year trends in cause-specific heart failure outcomes by sex, socioeconomic status, and place of diagnosis: a population-based study. Lancet Public Health. 2019 Aug;4(8):406–20. doi: 10.1016/S2468-2667(19)30108-2. https://linkinghub.elsevier.com/retrieve/pii/S2468-2667(19)30108-2 S2468-2667(19)30108-2 - DOI - PMC - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
