

Extending Thrombolysis in Acute Ischemic Stroke to Primary Care: Early Experiences with a Network-Based Teleneurology Approach
- PMID: 35225883
- PMCID: PMC8884013
- DOI: 10.3390/neurolint14010012
Extending Thrombolysis in Acute Ischemic Stroke to Primary Care: Early Experiences with a Network-Based Teleneurology Approach
Abstract
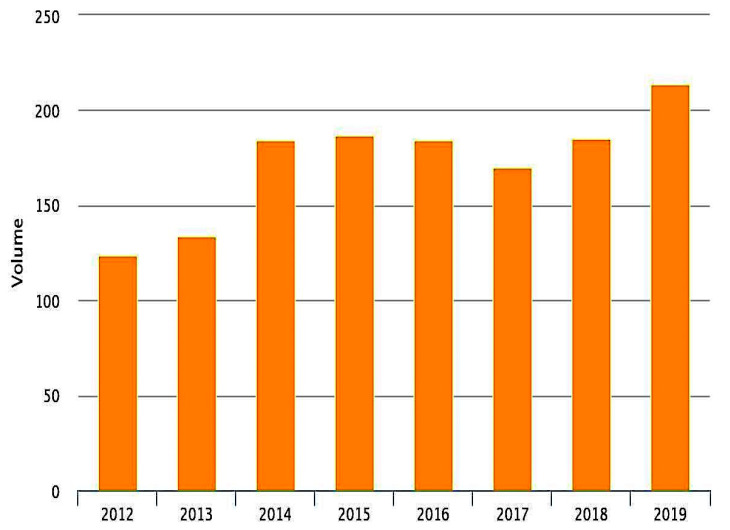
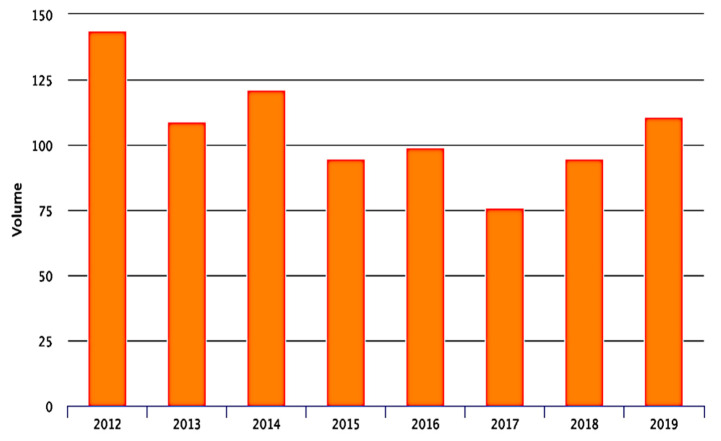
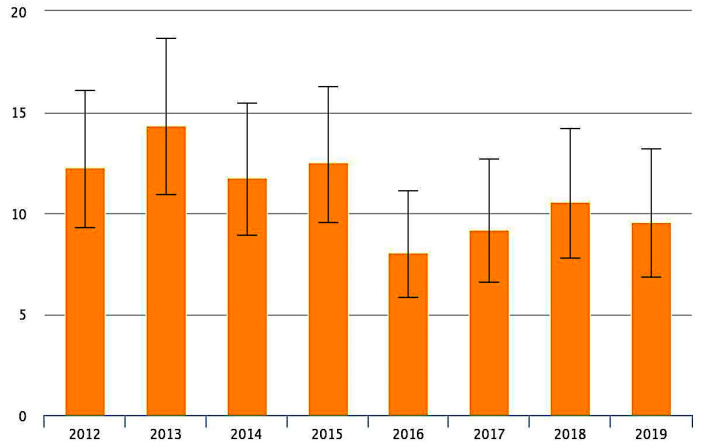
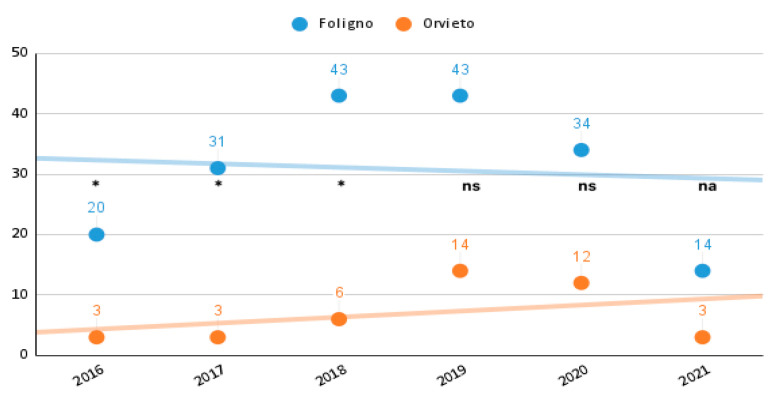
Background and Purpose-Systemic thrombolysis represents the main proven therapy for acute ischemic stroke, but safe treatment is reported only in well-established stroke units. To extend the use of tissue plasminogen activator (tPA) treatment in primary care hospitals on isolated areas through telemedic was the purpose of specific initiatives in southern Umbria, Italy. Methods-The stroke center of Foligno established a telestroke network to provide consultations for three local hospitals in southern Umbria. The telemedic system consists of a digital network that includes a two-way video conference system and imaging sharing. The main network hospital established specialized stroke wards/teams in which qualified teams treat acute stroke patients. Physicians in these hospitals are able to contact the stroke centers 24 h per day. Quality data are available to support the safe implementation of the stroke procedures. Those available from governmental authorities and local datasets are volume of hospitalization, in-hospital mortality, 30-days mortality, and discharge setting. Objective of the study was to assess the annual hospitalization volume in both the hub and spoke hospitals for ischemic stroke and appraise the performance of the network after the introduction of the telestroke system. Results-A total of 225 systemic thrombolyses were performed in time period indicated above all hospitals. In the main spoke hospital, 41 procedures were performed after teleconsultations were made available. The thrombolysis rate in the hub hospital ranged between 10% in 2016 and 20% in 2019, while in the spoke hospital was below 5% in 2016 and raised to 15% in 2019. The statistically significant difference, in the number of procedures, between hub and spoke in the beginning of the observation time disappeared after introduction of the telestroke network. No increase of the mortality was found. Conclusions-The present data suggest that systemic thrombolysis indicated via stroke experts in the setting of teleconsultation shows similar complication rates to those reported in the National Institute of Neurological Disorders and Stroke trial. Therefore, tPA treatment is also safe in this context and can be extended to primary hospitals.
Keywords: stroke; telemedicine; teleneurology; thrombolysis.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources
