

Survivorship, complications, and outcomes following distal femoral arthroplasty for non-neoplastic indications
- PMID: 35227074
- PMCID: PMC8965790
- DOI: 10.1302/2633-1462.33.BJO-2021-0202.R1
Survivorship, complications, and outcomes following distal femoral arthroplasty for non-neoplastic indications
Abstract
Aims: Endoprosthetic reconstruction with a distal femoral arthroplasty (DFA) can be used to treat distal femoral bone loss from oncological and non-oncological causes. This study reports the short-term implant survivorship, complications, and risk factors for patients who underwent DFA for non-neoplastic indications.
Methods: We performed a retrospective review of 75 patients from a single institution who underwent DFA for non-neoplastic indications, including aseptic loosening or mechanical failure of a previous prosthesis (n = 25), periprosthetic joint infection (PJI) (n = 23), and native or periprosthetic distal femur fracture or nonunion (n = 27). Patients with less than 24 months' follow-up were excluded. We collected patient demographic data, complications, and reoperations. Reoperation for implant failure was used to calculate implant survivorship.
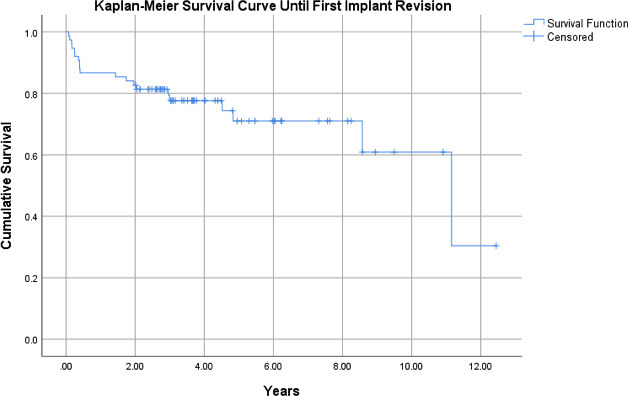
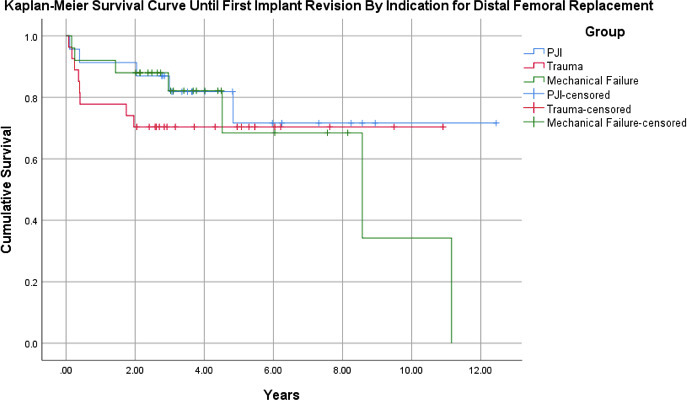
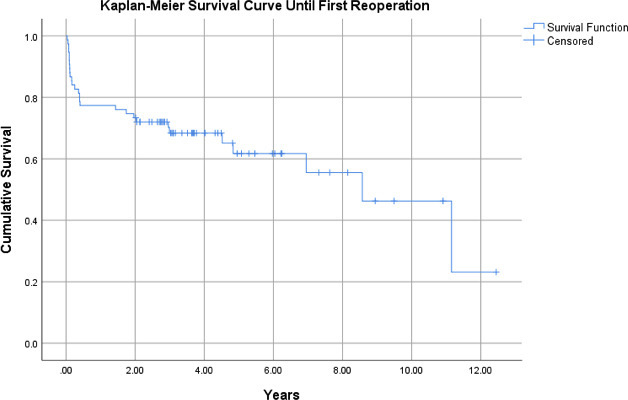
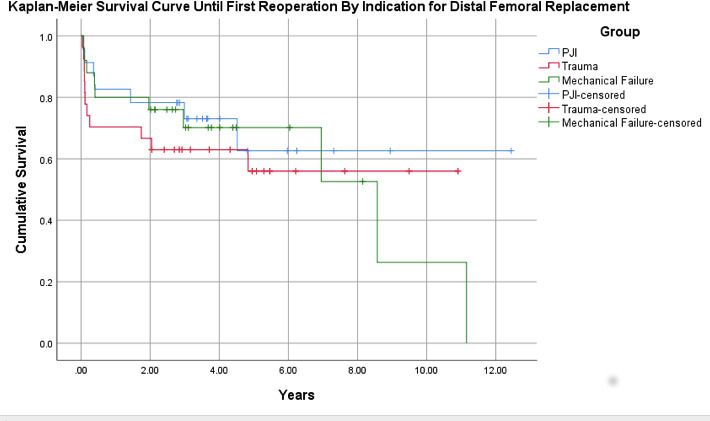
Results: Overall one- and five-year implant survivorship was 87% and 76%, respectively. By indication for DFA, mechanical failure had one- and five-year implant survivorship of 92% and 68%, PJI of 91% and 72%, and distal femur fracture/nonunion of 78% and 70% (p = 0.618). A total of 37 patients (49%) experienced complications and 27 patients (36%) required one or more reoperation. PJI (n = 16, 21%), aseptic loosening (n = 9, 12%), and wound complications (n = 8, 11%) were the most common complications. Component revision (n = 10, 13.3%) and single-stage exchange for PJI (n = 9, 12.0 %) were the most common reoperations. Only younger age was significantly associated with increased complications (mean 67 years (SD 9.1)) with complication vs 71 years (SD 9.9) without complication; p = 0.048).
Conclusion: DFA is a viable option for distal femoral bone loss from a range of non-oncological causes, demonstrating acceptable short-term survivorship but with high overall complication rates. Cite this article: Bone Jt Open 2022;3(3):173-181.
Keywords: Distal femoral replacement; Distal femur; Fracture; Mechanical failure; Megaprosthesis; Periprosthetic joint infection; Total joint; Trauma; aseptic loosening; distal femoral fractures; femoral arthroplasty; femoral bone loss; mechanical failure; nonunion; periprosthetic distal femur fractures; periprosthetic joint infection (PJI); reoperations; wound complications.
Figures
References
-
- Kurtz S, Ong K, Lau E, Mowat F, Halpern M. Projections of primary and revision hip and knee arthroplasty in the United States from 2005 to 2030. J Bone Joint Surg Am. 2007;89-A(4):780–785. - PubMed
-
- Kurtz SM, Ong KL, Schmier J, et al. . Future clinical and economic impact of revision total hip and knee arthroplasty. J Bone Joint Surg Am. 2007;89 Suppl 3(suppl_3):144–151. - PubMed
-
- Hamilton DF, Howie CR, Burnett R, Simpson A, Patton JT. Dealing with the predicted increase in demand for revision total knee arthroplasty: challenges, risks and opportunities. Bone Joint J. 2015;97-B(6):723–728. - PubMed
-
- Backstein D, Safir O, Gross A. Management of bone loss: structural grafts in revision total knee arthroplasty. Clin Orthop Relat Res. 2006;446:104–112. - PubMed
