

Adverse effects of delayed antimicrobial treatment and surgical source control in adults with sepsis: results of a planned secondary analysis of a cluster-randomized controlled trial
- PMID: 35227308
- PMCID: PMC8883454
- DOI: 10.1186/s13054-022-03901-9
Adverse effects of delayed antimicrobial treatment and surgical source control in adults with sepsis: results of a planned secondary analysis of a cluster-randomized controlled trial
Abstract
Background: Timely antimicrobial treatment and source control are strongly recommended by sepsis guidelines, however, their impact on clinical outcomes is uncertain.
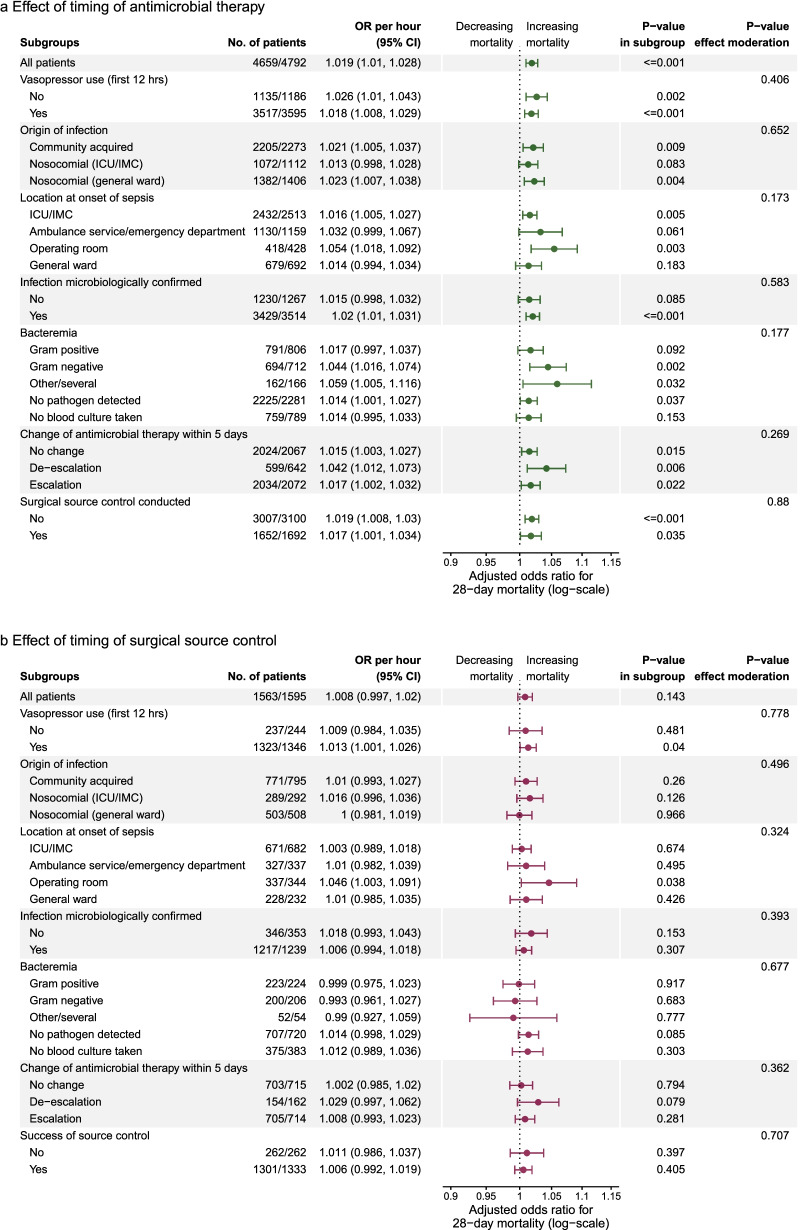
Methods: We performed a planned secondary analysis of a cluster-randomized trial conducted from July 2011 to May 2015 including forty German hospitals. All adult patients with sepsis treated in the participating ICUs were included. Primary exposures were timing of antimicrobial therapy and delay of surgical source control during the first 48 h after sepsis onset. Primary endpoint was 28-day mortality. Mixed models were used to investigate the effects of timing while adjusting for confounders. The linearity of the effect was investigated by fractional polynomials and by categorizing of timing.
Results: Analyses were based on 4792 patients receiving antimicrobial treatment and 1595 patients undergoing surgical source control. Fractional polynomial analysis identified a linear effect of timing of antimicrobials on 28-day mortality, which increased by 0.42% per hour delay (OR with 95% CI 1.019 [1.01, 1.028], p ≤ 0.001). This effect was significant in patients with and without shock (OR = 1.018 [1.008, 1.029] and 1.026 [1.01, 1.043], respectively). Using a categorized timing variable, there were no significant differences comparing treatment within 1 h versus 1-3 h, or 1 h versus 3-6 h. Delays of more than 6 h significantly increased mortality (OR = 1.41 [1.17, 1.69]). Delay in antimicrobials also increased risk of progression from severe sepsis to septic shock (OR per hour: 1.051 [1.022, 1.081], p ≤ 0.001). Time to surgical source control was significantly associated with decreased odds of successful source control (OR = 0.982 [0.971, 0.994], p = 0.003) and increased odds of death (OR = 1.011 [1.001, 1.021]; p = 0.03) in unadjusted analysis, but not when adjusted for confounders (OR = 0.991 [0.978, 1.005] and OR = 1.008 [0.997, 1.02], respectively). Only, among patients with septic shock delay of source control was significantly related to risk-of death (adjusted OR = 1.013 [1.001, 1.026], p = 0.04).
Conclusions: Our findings suggest that management of sepsis is time critical both for antimicrobial therapy and source control. Also patients, who are not yet in septic shock, profit from early anti-infective treatment since it can prevent further deterioration. Trial registration ClinicalTrials.gov ( NCT01187134 ). Registered 23 August 2010, NCT01187134.
Keywords: Anti-biotic agents; Infection control; Patient care bundles; Sepsis; Surgical source control; Time-to-treatment.
© 2022. The Author(s).
Conflict of interest statement
Dr. Rüddel has nothing to disclose. Dr. Bloos reports grants from German Federal Ministry of Education and Research to his institution, during and outside the conduct of the study; personal fees from Baxter, outside the submitted work, and receipt of kits for a clinical trial from Assoc. of CapeCods, outside the submitted work. Dr. Thomas-Rüddel reports grants from BMBF to his institution, outside the submitted work..Dr. Reinhart is shareholder with less of 0.5% of InflaRx NV a Jena /Germany based Biotech Company that evaluates a immunmodulatory approach for the adjunctive treatment of COVID-19. Dr. Bach has nothing to disclose. Dr. Gerlach has nothing to disclose. Dr. Lindner has nothing to disclose. Dr. Marshall reports consulting fees from Gilead Pharma, support for traveling to the WHO Covid-19 meeting by Bill and Melinda Gates Foundation, personal fees from AM Pharma for participation on a data safety monitoring board, being chair of the International Forum for Acute Care Trialists (unpaid), and being co-chair of the WHO Working Group on Clinical Characterization and Management of Covid-19 (unpaid), all outside the submitted work. Dr. Simon has nothing to disclose. Dr. Weiss has nothing to disclose. Dr. Schwarzkopf reports grants from German Federal Ministry of Education and Research to his institution, during the conduct of the study.
Figures


References
-
- Evans L, Rhodes A, Alhazzani W, Antonelli M, Coopersmith CM, French C, Machado FR, McIntyre L, Ostermann M, Prescott HC, et al. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock 2021. Intensive Care Med. 2021;47(11):1181–1247. doi: 10.1007/s00134-021-06506-y. - DOI - PMC - PubMed
-
- Rothrock SG, Cassidy DD, Barneck M, Schinkel M, Guetschow B, Myburgh C, Nguyen L, Earwood R, Nanayakkara PWB, Nannan Panday RS et al. Outcome of immediate versus early antibiotics in severe sepsis and septic shock: a systematic review and meta-analysis. Ann Emerg Med. 2020. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
